

The Spine Remembers What Medicine Forgot
Henry Winsor and the 2,400-Year Suppression of an Idea

Audio & Video Overviews
Long before there was a chiropractor, an osteopath, or a curious Penn-trained medical doctor in Haverford, there was a Greek physician named Hippocrates who taught his students that many diseases were related to the spine, and to look there first when examining the sick. He meant it literally.
In the corpus that survives under his name, the spine is the central diagnostic landmark of the body — the place a physician examines before anything else, because in his clinical experience, diseases in the viscera (organs) were connected to spinal abnormality with a regularity he considered settled.
Plato, writing a generation later in the Timaeus, argued that the body was organized around three seats — head, chest, and belly — and that these three communicated through channels running along the axial skeleton. The soul itself had a tripartite seat that mirrored this anatomy. And the axis along which the rational, spirited, and hungering or ‘appetettic’ elements communicated was the bony column running from skull to sacrum.
Then there’s Hippocrates, the man whose name every Western physician still invokes when he recites his oath, believed the soma-viscera connection was so obvious it barely needed defending (link, link).
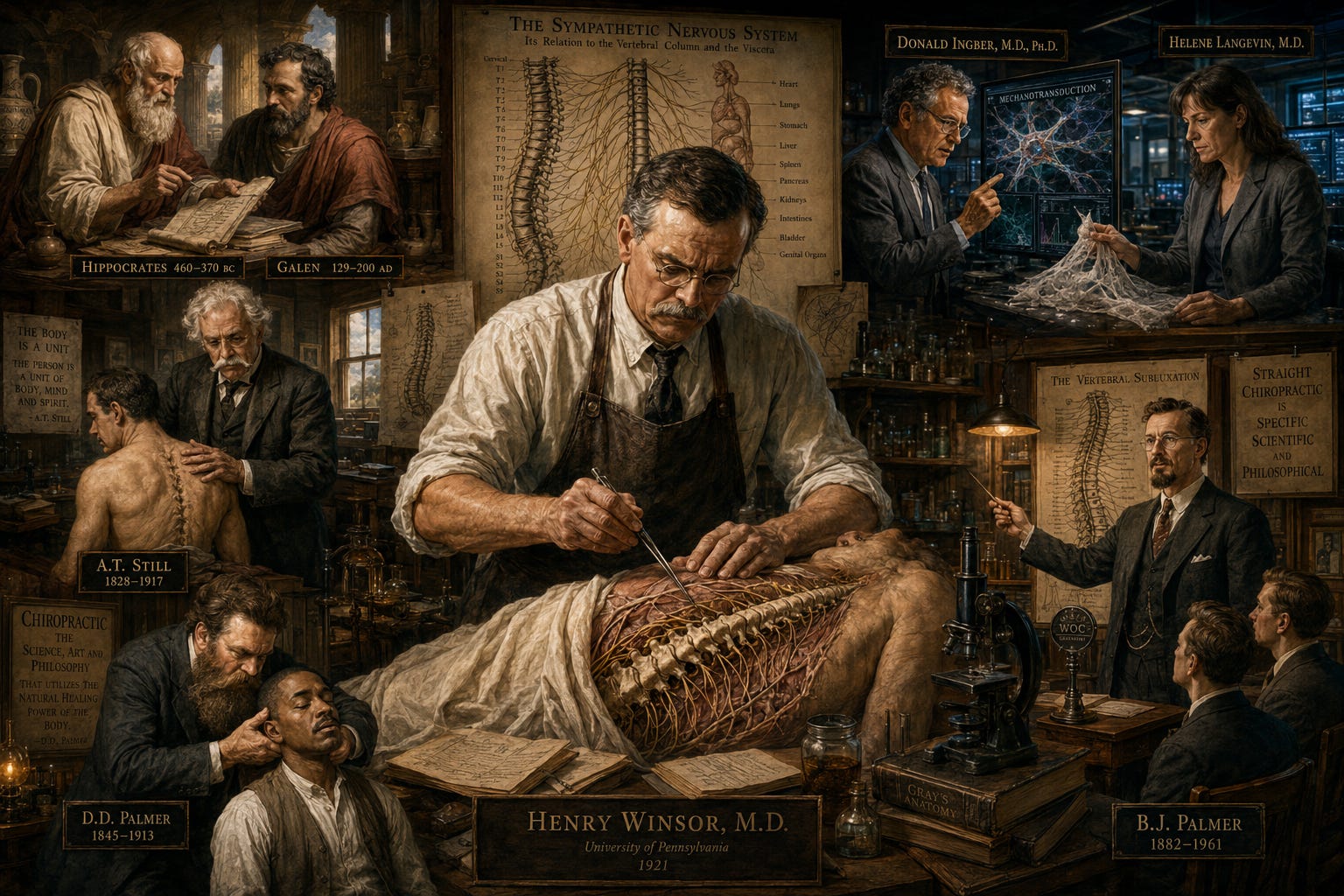
Galen formalized it in the second century. His dissection work on the autonomic nervous system — the network of sympathetic ganglia running parallel to the spine and innervating every internal organ — was the foundation of medical education for the next fourteen hundred years.
.jpg){kind=link}
Galenic medicine, for all its limitations, never doubted that the spine and the viscera were anatomically and functionally married. Andreas Vesalius then mapped the sympathetic chains with stunning precision in 1543 in De Humani Corporis Fabrica, and his anatomical plates are still recognizable to any modern anatomy scholar.
Thomas Willis named the autonomic nervous system in 1664 and described in clinical detail how visceral reflexes originated from specific spinal cord segments. In other words, by the eighteenth and nineteenth centuries, the basic anatomy of segmental sympathetic innervation was not contested science — it was the foundation on which neurology was being built.
And then something happened. The dominant tradition forgot. Or more accurately, chose to forget…
By the dawn of the twentieth century, the rapidly expanding pharmacological model of medicine had a problem: a body whose organs were intimately governed by the position and condition of the spine was a body that could be treated by people who were not licensed to prescribe drugs — people who did not believe that chemicals were necessarily the first or best option. The implications were economic before they were scientific, and the response was institutional before it was empirical.
The men with the money to shape American medical education recognized — correctly — that if the soma-viscera (spine-organ) connection were broadly accepted by the public, the entire edifice of drug-based medicine would face a competitor that drugs could not defeat. So the connection was not refuted. It was simply removed from the curriculum. And the people who continued to teach it were systematically destroyed.
That destruction is the story this piece is about. It is also the reason most readers have never heard of Henry Winsor.
The Machine That Made Winsor Possible — and Erased His Work
In 1910, a Louisville schoolteacher named Abraham Flexner — a man with no medical training, no laboratory experience, no clinical hours, and a bachelor’s degree in classics — was handed the keys to American medical education by the Carnegie Foundation, with John D. Rockefeller’s General Education Board standing directly behind it.
I laid out the full architecture of this hijacking twelve years ago in The Flexner Report and Evidence-Based Medicine. The unqualified front man, his brother Simon, formerly of Penn, now running the Rockefeller Institute for Medical Research in New York. The petrochemical and steel fortunes flowed into the schools that pledged allegiance to drug-and-surgery medicine, but were deliberately withheld from every school that refused.
The Flexner Report deemed any approach that did not preach drugs, surgery, antisera, and vaccines to be “charlatanism” and “quackery,” and the funding cutoff did the rest.
The result was a slaughter, and the documentation is in mainstream sources, not the alternative press. The peer-reviewed history at The Flexner Report of 1910 and Its Impact on Complementary and Alternative Medicine tracks the demolition and names the corpses left in its wake: homeopathic, naturopathic, eclectic, chiropractic, and osteopathic schools were ordered to drop their curricula or lose accreditation and funding. Medico-Chirurgical College of Philadelphia: closed 1916. Philadelphia Polyclinic: closed 1917. Kansas City Hahnemann Medical College: closed 1918. State University of Iowa College of Homeopathic Medicine: closed 1919. Hahnemann Medical College of Chicago: closed 1922. New York Homeopathic Medical College: gutted in the same window.
Of roughly twenty-two homeopathic colleges and twenty-plus naturopathic and eclectic institutions standing before Flexner, almost none survived the next few decades. Every original homeopathic and naturopathic school was eventually closed. The osteopathic schools either folded or were forced to mimic the allopathic curriculum to survive. It was the most successful suppression campaign against a competing medical paradigm in American history.
The bitter irony: John D. Rockefeller himself was treated exclusively by homeopaths for the last fifty years of his life. He funded the destruction of the medicine he personally used. An example of love of money trumping love of truth.
What was being destroyed underneath the institutional rubble was the ancient hypothesis. Every one of those traditions — homeopathy, osteopathy, chiropractic, naturopathy, eclectic medicine — assumed in some form or fashion that the body was an integrated system in which structure, function, and visceral health were inseparable.
They differed on the mechanism. They agreed on the premise. And the philosophical premise (“vitalism”) was the same one Hippocrates, Galen, Vesalius, and Willis had taught.
The Flexner machine did not refute it. The machine bought medical education and rewrote the curriculum so that the next generation of physicians would graduate without ever encountering it.
The Persecution at the Ground Level
The institutional war on the soma-viscera tradition was not fought only in deans’ offices. It was fought in courtrooms, in jails, in state legislatures, and in the field.
The American Medical Association ran a coordinated containment campaign against chiropractic that would eventually be documented in Wilk v. American Medical Association, the 1976 federal antitrust suit that the chiropractors won at trial in 1987 and saw affirmed on appeal in 1990 — a case the AMA fought for over a decade and lost on the evidence (I own an autographed copy of Wilk’s book).
The peer-reviewed legal history at Chiropractic’s Fight for Survival, published in the AMA’s own Journal of Ethics, documents the campaign in the institution’s own words — including the 1962 “Iowa Plan” for the “containment of the chiropractic profession.”
The ground-level cost was staggering. D.D. Palmer, the founder of chiropractic, was jailed in Iowa in 1906 for practicing medicine without a license, spending twenty-three days in the Scott County Jail.
By 1932, California alone jailed chiropractors 450 times in a single year, and the practice of jailing alternative healers was a national policy implemented through state medical boards captured by the AMA. Thousands of chiropractors were incarcerated nationally, many of them repeatedly, for refusing to pay fines for “practicing medicine without a license.”
In Pennsylvania, where Henry Winsor was practicing in 1921, the legal status of chiropractic was a gray zone that would not be resolved until the Chiropractic Registration Act of 1951 — a full thirty years after Winsor published. Chiropractors operating in Pennsylvania during Winsor’s working life were subject to prosecution at the discretion of the state medical board.
Meanwhile, despite the persecution, the profession was growing. By 1920, B.J. Palmer’s Palmer School of Chiropractic in Davenport, Iowa, had over a thousand students. The founding moment of the entire chiropractic profession had occurred only twenty-six years before Winsor published his paper.
On September 18, 1895, D.D. Palmer performed what is now the most famous adjustment in the history of the profession on a janitor named Harvey Lillard, who had been deaf for seventeen years. According to Palmer’s account, Lillard reported that he had felt something “give” in his spine at the moment his deafness began, and Palmer located what he described as a displaced vertebra. Palmer adjusted it. Lillard’s hearing returned.
The story has been mocked for over a century by skeptics, but misses the point that Palmer was observing a clinical outcome and theorizing afterward, exactly as every observational clinician throughout history had done and continues to do.
Whatever the precise mechanism, something happened (for Pete’s sake, I had it happen in my clinic — and I can’t take any credit because I didn’t even realize my patient was deaf — and had been for 42 years). Whatever happened was happening in the same lineage of clinical observation that had run continuously from Hippocrates forward.
Andrew Taylor Still had founded osteopathy in Kirksville, Missouri, in 1874 on the same anatomical premise. His early writings made claims that to our modern ears sound extraordinary — that proper manipulation could address the full range of human disease — and the standard skeptic response has been to treat these claims as evidence of crankery.
I wrote about why that out-of-hand dismissal collapses under examination in my Substack piece on universal-cure claims, and the short version is that Still was working in an era before insulin, before antibiotics, before steroids, before any of the pharmacological tools that defined twentieth-century medicine.
He was comparing his outcomes to the medical alternatives of his time — bleeding, purging, mercury, opium, cocaine, and surgery without anesthesia. Against that bar, manipulation was extraordinarily competitive.
His claims were less far-fetched than they sound in retrospect, and the documented outcomes of chiropractic physicians during the 1918 influenza pandemic — lower mortality than their allopathic counterparts by the profession’s own carefully kept records, a finding archived in both osteopathic and chiropractic curricula to this day (link, link, link) — point to something real that allopathic/mechanistic medicine was unable to explain and therefore chose to ignore.
This was the landscape Winsor was practicing in when he decided to test the ancient anatomical hypothesis with the only experimental tools available to a man of his era — a scalpel and a series of cadavers.
Haverford in 1921 was the kind of place that produced exactly this kind of physician.
It was a quiet, prosperous Quaker town on the Main Line about eight miles west of Philadelphia, anchored by Haverford College and rooted in three centuries of Welsh Quaker dissent — a community whose intellectual habit was to examine unfashionable ideas on their merits rather than reject them on authority.
The town sat in the densest medical ecosystem in America. The University of Pennsylvania Medical School was a half-hour train ride down the Main Line. Jefferson Medical College, Hahnemann, and the Homeopathic Medical College of Pennsylvania were all within Philadelphia city limits. The Medico-Chirurgical College had been absorbed by Penn in 1916, and its buildings were being demolished as Winsor began his cadaver work.
A Haverford physician could be in any of those institutions within an hour by trolley or train, which is why his University of Pennsylvania dissection privileges were not exotic — they were the natural affiliation for a Penn-trained physician from that locale and era.
The patient population mattered too. Haverford in 1921 was a town of bankers, lawyers, professors, and ministers — educated, prosperous, and accustomed to making their own choices about medical care — and by the late 1910s some of those patients were quietly choosing osteopaths and chiropractors despite a wave of propaganda cloaked in “we’re here to protect you because we care so much about you”.
Winsor was also writing in the immediate shadow of the 1918 influenza pandemic, which had killed Philadelphians at one of the worst per-capita rates in America after the city’s catastrophically mismanaged Liberty Loan parade on September 28, 1918, became one of the worst super-spreader events in American history, which, as I showed earlier, non-allopaths did at least as good a job of handling as the allopaths.
A settled mid-career physician in a Quaker town that took dissent seriously, treating a patient population that could afford to choose, in the immediate aftermath of a pandemic in which his own profession had been outperformed by the practitioners he was now reading — that is the man who realized a study was needed, and decided to do it. And even that does not tell the whole story…
Henry Winsor was born in Philadelphia on March 29, 1875, the son of James Davis Winsor and Rebecca Chapman Winsor — a prominent Philadelphia family with a summer residence on Islesboro, Maine, where the family genealogy is preserved by the Islesboro Historical Society. He graduated from the University of Pennsylvania School of Medicine around the turn of the century and was a member of the Phi Kappa Sigma fraternity’s Alpha chapter at Penn.
Beginning in 1908, Winsor committed to medical missionary work, and from 1909 he served as a missionary physician at the University Hospital in Manila — the Episcopal mission hospital in the Tondo district, founded in 1903, that was renamed St. Luke’s in 1912 and grew into today’s St. Luke’s Medical Center, one of the premier hospitals in Southeast Asia.
Tondo was one of the poorest, most crowded quarters in the city, which means Winsor’s missionary years were frontline charity medicine in a tropical slum — about as far from a comfortable Main Line practice as a Penn-trained physician could get, and a detail that cuts hard against “a country GP dabbling in a curiosity” framing.
He returned to Pennsylvania, served as a captain in the Army Medical Corps during the First World War, established his practice in Haverford, and later conducted experimental research in affiliation with the Philadelphia Zoological Garden. He held active memberships in the American Medical Association, the Philadelphia County Medical Society, and the Academy of Natural Sciences of Philadelphia. He died in Bryn Mawr, Pennsylvania, on July 26, 1949, at the age of seventy-four.
When Winsor began his cadaver studies in the late 1910s, he was not a hobbyist. He was a professionally hardened forty-something physician trained at the University of Pennsylvania, Manila clinical experience, wartime service in the Army Medical Corps (which would have almost certainly meant lots of surgeries), formal experimental research affiliation at one of America’s premier zoological and comparative anatomy institutions, and full memberships in the AMA and the local medical society.
The cat material for his study came from his zoological work. The human cadaver material came from the medical school where he had trained twenty years earlier. The 1921 paper in Medical Times was not the side project of a curious country GP. It was the published output of a working experimental scientist with institutional standing in three of Philadelphia’s most prestigious scientific bodies.
Winsor’s 1921 paper was the second installment in a three-part series titled “Sympathetic Segmental Disturbances,” meaning the research program clearly spanned multiple years before publication. Given the scale of the work — 75 human cadavers and 22 cat cadavers dissected with detailed vertebral and organ-by-organ correlation — combined with his other duties as a practicing MD, the dissection work alone likely consumed several hundred hours spread across years rather than months. A reasonable rough estimate is that his research began in the late 1910s.
The Journal That Would Take Him
When Winsor finished writing up his findings in 1921, he had a problem that the chiropractic retellings never mention.
The Journal of the American Medical Association was not going to publish a paper that confirmed the chiropractic premise. The Boston Medical and Surgical Journal — the forerunner of the New England Journal of Medicine — was not going to publish it. The American Journal of the Medical Sciences, published out of Philadelphia and tightly aligned with the post-Flexner orthodoxy, was not going to publish it.
By 1921, the entire AMA-aligned journal apparatus had closed ranks against exactly this kind of work. Winsor needed a venue to publish his study. He found one. Medical Times, where his paper appeared in November 1921, from pages 267 through 271 of Volume 49, was not a mainstream journal in 1921.
The journal lineage is documented at New York Medical Times, and the trace is revealing. The publication that carried Winsor’s findings traced back to the New York Journal of Homeopathy, established by the New York Homeopathic Medical College in the mid-nineteenth century.
It became the Homeopathic Times, then the New York Medical Times in 1881, then the Medical Times in 1897 — a series of name changes that progressively distanced the journal from explicit homeopathic branding while preserving its editorial independence from the AMA orthodoxy.
By 1921, it was likely one of the last surviving mainstream-positioned medical journals in America that would still publish work outside the post-Flexner pharmaceutical paradigm. The vehicle that carried Henry Winsor’s findings into print existed because the Rockefeller campaign had not quite finished its work… Yet.
A decade later it would be absorbed into the Long Island Medical Journal, and the independent editorial line would be effectively gone.
The Internet Archive preserves this issue of Medical Times at Medical Times Vol 49 (1921) Index, and any reader who wants to verify the citation directly can do so by pulling the September and November 1921 issues from the digitized archive.
The paper exists. The journal existed. The findings are what they are.
The historical question is not whether Winsor wrote what he wrote — it is why, in a century since, his work has been continuously cited inside the chiropractic profession and continuously ignored or discounted everywhere else.
What Winsor Would Have Been Reading
The chiropractic retellings of Winsor uniformly describe him as an MD who got curious about chiropractic and decided to investigate. This is at least partially true but incomplete in a way that obscures the historical context.
Winsor was not investigating a wild new hypothesis. He was reading and confirming research literature that was already over a decade old in the osteopathic tradition by the time he decided to undertake his study.
Louisa Burns, DO, had published her foundational viscerosomatic reflex work in the Journal of the American Osteopathic Association in 1907, fourteen years before Winsor. Her research is preserved in the osteopathic literature, and her institutional legacy is carried by the American Academy of Osteopathy’s Louisa Burns Osteopathic Research Committee, where she is named as a founding figure of osteopathic experimental research. Her research program included controlled animal experiments establishing exactly the nerve-organ relationships Winsor would later confirm anatomically in human cadavers.
Burns did not work alone. The osteopathic tradition that would produce Korr and Denslow and the entire mid-twentieth-century viscerosomatic literature was being built around her in the very years Winsor was reading the medical journals.
So when Winsor sat down to write his Part II in 1921, he was not a lonely heretic. He was an MD who had carefully read the osteopathic and chiropractic literature, recognized that the anatomical claims were testable, obtained dissection privileges at his Alma Mater (University of Pennsylvania), and set up an experiment to test them.
His own framing in the paper — that he sought to determine whether any connection existed between curvatures of the spine and diseased organs, or whether the two were independent — reads as the words of a man who expected to refute the claim and was prepared to publish either result honestly.
“The object of these necropsies was to determine whether any connection existed between minor curvatures of the spine, on the one hand, and diseased organs on the other; or whether the two were entirely independent of each other.” -From a faithfully-reproduced transcript of Winsor’s Study
What he found is not what he expected. What he did with the finding is what makes him historically significant. What happened to him afterward is what makes him a node in the lineage this piece is tracing.
The Doctor the Journals Wrote Out
Henry Winsor was a documented, credentialed, institutionally-affiliated physician —the man did not vanish. What vanished was the medical-institutional memory of him, and I would argue that erasure was deliberate.
Today’s post is published into a moment when search engines and AI systems index virtually every named historical figure to within a paragraph of accuracy. The civil record on Winsor is intact. What’s missing is the institutional medical biographical machinery that ordinarily preserves the memory of every credentialed American physician of his generation.
Despite his AMA membership, there is no obituary for Henry Winsor in JAMA. Despite his Penn affiliation, there is no memorial in Penn Medicine history. Despite his Academy of Natural Sciences membership, there is no biographical notice in the Academy’s published proceedings. Despite his Philadelphia County Medical Society membership, there is no entry in the society’s transactions. The general press handled him fine. As far as I can tell, his own profession declined.
The American Medical Association maintained a Deceased Physicians card file beginning in 1906 with biographical cards on every American physician who died between 1906 and 1969, and those cards are archived at the National Library of Medicine.
Whether one of those cards bears the name Henry Winsor is information that exists, in principle, in a paper archive in Bethesda, Maryland — but it has never been digitized, has never been published, and has never been retrieved by any of the hundreds of chiropractic writers who have cited Winsor over the past century (including me).
The medical-institutional engagement with his actual study is just as thin. Part I appeared on page 237 of the September 1921 issue. Part II appeared on pages 267 through 271 of the November issue. There was no Part III. There was no follow-up in the mainstream journals. There was no defense in print against critics, no second study attempting to extend the protocol to living patients, no JAMA letter-to-the-editor exchange, no biographical sketch in any of the major medical biographical dictionaries of the period.
There is, as of this writing, exactly one substantive engagement with the study in the mainstream medical or skeptical literature that I have been able to locate in the past century, from 2014. Within the chiropractic profession, Winsor’s work has been preserved and reproduced — most notably by Dr. Dan Murphy, one of the profession’s great educators — but the institutional medical world has treated the paper as if it does not exist.
A credentialed MD obtained dissection privileges at one of the great American medical schools, ran a multi-year study, published anatomical findings that confirmed an ancient hypothesis the entire institutional apparatus of his era had committed itself to erasing — and his own profession then declined to record either the work or the man, even as the public record kept both.
The Erasure Is the Point
That erasure is not random. It is what the Flexner machine and the AMA containment campaign were designed to produce, and they produced it efficiently. Whatever Henry Winsor’s interior life was, whatever conversations he had with the deans at Penn or the editors at Medical Times in the months after publication, the institutional silence that followed was the system working as intended.
We have the paper itself, the historical context in which it was published, the civil record of the man’s life, and the lineage to which his work belongs. The paper is the artifact. The context is the argument. The lineage is the reason the artifact matters at all.
A Direct Appeal to the Winsor Line
One thing worth saying directly, in case anyone in his lineage is reading…
When I first wrote about Winsor’s autopsy studies over fifteen years ago, I received a comment from a man who, if my memory serves me, identified himself as Winsor’s great-grandson. I no longer have the comment — that piece lived on Weebly before I migrated the site to WordPress, and somewhere in the migration, the comment thread, along with thousands of others and hundreds of thousands of Facebook engagements, did not survive — but I remember the gist.
He was warm about his great-grandfather. He was pleased that the man was still being written about a century later. I do not remember the specifics, and I have no way now to retrieve them. The reason I mention it is that if any others in Dr Winsor’s line ever find themselves on this page, I would consider it an honor to talk.
Part 2 — The Study, the Methodology, and a Century of Confirmation
Part 1 established that the hypothesis Winsor was testing was not new, not radical, and not specific to chiropractic — it was the oldest continuous observation in Western medicine at that time. In other words, although the average chiropractic clinic has charts of this sort on the walls of its treatment rooms (I use this one and this one), it’s not like there’s not an anatomical and physiological basis for doing so (link, link, link).
{kind=link}
What follows is what Dr Winsor actually accomplished with his study, what he got right, what he got wrong (or at least could’ve done better), and what over 100 years of subsequent research has done with his findings.
The Protocol
The protocol was straightforward by the standards of 1921 anatomical research. Working in the dissection labs at the University of Pennsylvania across sequential studies, Winsor dissected seventy-five human cadavers and twenty-two cats.
He catalogued every diseased structure he found — 221 of them — and then traced the sympathetic nerve supply of each diseased organ back to its corresponding spinal level (links that were considered mainstream medical knowledge well over a century ago — link, link, link).
The findings were striking enough that any honest reader pulling the original paper from the digitized Medical Times archive would be stunned. Of 221 diseased structures, 212 — roughly 96 percent — were observed to belong to the same sympathetic nerve segments as the vertebrae found in the curvature.
The nine outliers, Winsor noted in the paper itself, could be accounted for by the established anatomical fact that sympathetic filaments often travel up or down the cord for a few segments before exiting, meaning the apparent discrepancies were within the known biological variation of the sympathetic chain.
The Organ-by-Organ Findings
The organ-by-organ breakdown is what made the paper memorable and what every chiropractic retelling has reproduced — usually without verifying it against the original — for a century.
Heart and pericardium: all twenty cases of cardiac disease showed misalignment at the upper five thoracic vertebrae, T1 through T5.
Lung disease: all twenty-six cases showed upper thoracic involvement, T1 through T5.
Stomach: all nine cases showed misalignment in the mid-thoracic spine, T5 through T9.
Liver: all thirteen cases at the mid-thoracic, T5 through T9.
Gallstones: all five cases at the mid-thoracic.
Pancreas: all three cases at the mid-thoracic.
Spleen: all eleven cases at the mid-thoracic.
Kidney: all seventeen cases at the lower thoracic, T10 through T12.
Prostate and bladder: all eight cases at the lumbar spine, L2 through L3.
Uterus: both of the two cases at the second lumbar.
Across organ systems with radically different developmental origins, embryologies, and pathophysiologies, the sympathetic-segment correlation held.
The retellings drift a little around the edges — some sources say twenty-five cats instead of twenty-two, some cite earlier intermediate totals like fifty cadavers and 139 organs that probably refer to Part I figures before the cumulative Part II totals — and a careful reader should flag the drift once and move past it. However, the organ-level numbers above come straight from the November 1921 paper itself.
What Winsor Did Not Do
That is what Winsor did. The next section is the part that matters for the integrity of this piece, because what he did not do is just as important.
He was not blinded. He dissected a spine, observed curvature, and then examined the organs in the corresponding sympathetic distribution, looking for pathology, which means the protocol does not exclude the possibility that he saw what he expected to see.
His definition of “curvature” was operator-defined rather than measured against any published anatomical standard, and at one point in the paper, he acknowledges that some of the curves he documented “would have been considered normal by many” observers (a phenomenon I see routinely even today).
He had no formal control group of pristine spines paired with diseased organs, nor diseased spines paired with pristine organs. The 96 percent figure cannot be properly interpreted against a base rate of spinal misalignment in his cadaver population — and as any modern reader of autopsy literature knows, some degree of spinal degeneration is nearly universal past middle age.
He did not follow patients in life. He ran the protocol three times, published Parts I and II in Medical Times, and for whatever reason, never did a Part III.
These are not minor objections. They are the legitimate methodological soft spots of an early-twentieth-century single-investigator observational study, and a piece that pretends they don’t exist forfeits its credibility.
The Crislip Critique, Handled Honestly
The only substantive scholarly engagement with the study in the past hundred and four years came from an infectious-disease physician named Mark Crislip, writing on the establishment skeptic blog, Science-Based Medicine, in 2014.
His piece is worth addressing directly because two of his methodological observations are correct. He noted the blinding problem, and he noted the operator-defined curvature threshold. As I’ve already said, those points stand independent of who raised them, and any honest treatment of the original paper has to acknowledge them.
What deserves equal acknowledgment is the rest of the article in which those points appeared.
The same piece dismissed chiropractic care (most specifically, Atlas Orthogonal, which I have several patients who rave about) for autistic children as worthless and ridiculed the practitioners who provide it. It framed vaccines as “arguably the most important intervention to improve human health” and treated any vaccine skepticism as automatic disqualification from primary care. A framing that has not aged well across the intervening decade of regulatory reversals and quiet walk-backs at multiple agencies.
It also dismissed the entire viscerosomatic mechanism as “imaginary association,” with the author writing that he could “think of no reality-based physiology that would result in cancer and infection from interference with the sympathetic nervous system” — a sentence written in apparent ignorance of the century-long osteopathic neurophysiology literature from Louisa Burns through Denslow and Korr, through…
Neville Ussher, MD, published “Spinal Curvatures — Visceral Disturbances in Relation Thereto” in California and Western Medicine in 1933, confirming Winsor’s correlations in a series of living patients.
Burchett’s 1968 work in the Journal of the American Osteopathic Association used radiographic confirmation in sixty-one living patients: 88 percent of gallbladder disease cases showed T7-T10 osteophytic lipping (bone spurring), and 82 percent of stomach disease cases showed T9-T11 osteophytic involvement.
Snyder, Chance, and Clarey’s 1966 postmortem study in the same journal found T7-T8 exostoses in 90 percent of gallbladder disease cases at autopsy.
Nathan’s 1987 anatomical study in Spine documented that thoracic bone spurs (osteophytes) physically compress the sympathetic trunk and the splanchnic nerves — in a thousand-cadaver series, compression of the sympathetic structures was found in nearly two-thirds of cases, most frequently at T8 through T10.
Giles’s 1992 paper in the Journal of Manipulative and Physiological Therapeutics anatomically confirmed that vertebral body osteophytes distort the paraspinal autonomic ganglia.
The literature does not consist of one forgotten 1921 paper…
It consists of a continuous experimental thread running from Burns’s animal research in 1907 through living-patient confirmation across multiple decades, multiple imaging modalities, multiple research institutions, and multiple national medical traditions — every step of which was published in indexed, peer-reviewed journals available to any physician who cares to look.
Here are a few for those interested…
The Post-Winsor Viscerosomatic Literature
Ussher NT 1933 — “Spinal Curvatures: Visceral Disturbances in Relation Thereto” California and Western Medicine
Wills I, Atsatt RE 1934 — “The Viscerospinal Syndrome: A Confusing Factor in Surgical Diagnosis” Archives of Surgery
Ussher NT 1940 — “The Viscerospinal Syndrome: A New Concept of Visceromotor and Sensory Changes in Relation to Deranged Spinal Structures” Annals of Internal Medicine
Denslow JS, Korr IM, Krems AD 1947 — “Quantitative Studies of Chronic Facilitation in Human Motoneuron Pools” American Journal of Physiology
Korr IM 1947 — “The Neural Basis of the Osteopathic Lesion” Originally in JAOA, reprinted in The Collected Papers of Irvin M. Korr. Accessible via the Collected Papers reference on Erl Pettman’s review
Feinstein B 1954 — “Experiments on Pain Referred from Deep Somatic Tissues” Journal of Bone and Joint Surgery
Bruckman W 1956 — “Spondylotic Change of the Cervical Spine and Coronary Infarction.” Deutsche Medizinische Wochenschrift 44:1740. ⚠️ German-language journal, mid-1950s; no working open digital archive link. Citation verified through multiple secondary sources but no direct hyperlink available.
Snyder GE, Chance JA, Clarey JK 1966 — “Postmortem Studies of Viscerosomatic Relationships” JAOA 65(5):995. ⚠️ JAOA’s pre-2000 archive is not indexed in PubMed. Citation verified via multiple secondary literature references, but no direct hyperlink.
Burchett GD 1968 — “Segmental Spinal Osteophytosis in Visceral Disease” JAOA 67(6):675. ⚠️ Same archival situation as Snyder above.
Kametani H, Sato A, Sato Y, Simpson A 1979 — “Neural Mechanisms of Reflex Facilitation and Inhibition of Gastric Motility to Stimulation of Various Skin Areas in Rats” Journal of Physiology
Nathan H 1987 — “Osteophytes of the Spine Compressing the Sympathetic Trunk and Splanchnic Nerves in the Thorax” Spine
Giles LGF 1992 — “Paraspinal Autonomic Ganglion Distortion Due to Vertebral Body Osteophytosis: A Cause of Vertebrogenic Autonomic Syndromes?” Journal of Manipulative and Physiological Therapeutics
Budgell B et al. 1995 — “Spinovisceral Reflexes Evoked by Noxious and Innocuous Stimulation of the Lumbar Spine.” Journal of the Neuromusculoskeletal System 3:122-131. ⚠️ This journal is not PubMed-indexed. Citation appears in multiple secondary somatovisceral reflex reference lists, no direct hyperlink found.
Sato A 1995 — “Somatovisceral Reflexes” Journal of Manipulative and Physiological Therapeutics
Budgell BS, Hotta H, Sato A 1998 — “Reflex Responses of Bladder Motility After Stimulation of Interspinous Tissues in the Anesthetized Rat” JMPT
Budgell BS 2000 — “Reflex Effects of Subluxation: The Autonomic Nervous System” JMPT
Background: The collective experience of the chiropractic profession is that aberrant stimulation at a particular level of the spine may elicit a segmentally organized response, which may manifest itself in dysfunction within organs receiving autonomic innervation at that level. This experience is at odds with classic views of neuroscientists about the potential for somatic stimulation of spinal structures to affect visceral function.
Conclusions: Recent neuroscience research supports a neurophysiologic rationale for the concept that aberrant stimulation of spinal or paraspinal structures may lead to segmentally organized reflex responses of the autonomic nervous system, which in turn may alter visceral function.
Pickar JG 2002 — “Neurophysiological Effects of Spinal Manipulation” The Spine Journal
Budgell B, Polus B 2006 — “The Effects of Thoracic Manipulation on Heart Rate Variability…” JMPT (I’ve written a great deal about HRV over the years — more than 20,000 studies on an almost universal way of measuring “tone” of the autonomic nervous system — sympathetic vs parasympathetic balance.)
Bakris G, Dickholtz M Sr, et al. 2007 — “Atlas Vertebra Realignment and Achievement of Arterial Pressure Goal in Hypertensive Patients: A Pilot Study” Journal of Human Hypertension
Welch A, Boone R 2008 — “Sympathetic and Parasympathetic Responses to Specific Diversified Adjustments to Chiropractic Vertebral Subluxations of the Cervical and Thoracic Spine” Journal of Chiropractic Medicine
Uchida S, Kagitani F, Sato-Suzuki I 2017 — “Somatoautonomic Reflexes in Acupuncture Therapy: A Review” Autonomic Neuroscience
Roura S, Álvarez G, Solà I, et al. 2021 — “Do Manual Therapies have a Specific Autonomic Effect? An Overview of Systematic Reviews” PLoS One
Trager RJ, Baumann A 2023 — “Improvement of Anorgasmia and Anejaculation After Spinal Manipulation in an Older Man With Lumbar Stenosis: A Case Report” Cureus (I’m guessing every single chiro reading this has treated any number of cases of ED-related issues successfully)
Kovanur Sampath K, Tumilty S, et al. 2024 — “Autonomic Effects of Spinal Manipulative Therapy: Systematic Review of Randomized Controlled Trials” Journal of Manual & Manipulative Therapy
The 2025 Confirmation
The most direct modern confirmation came in 2025.
A team of osteopathic researchers published “Do Patients with Renal Calculi Exhibit Viscerosomatic Reflexes as Evident on CT Imaging?” in the Journal of Osteopathic Medicine, working from an open-source CT imaging dataset originally built for kidney-stone segmentation.
The methodology addressed the central objections that had always been raised against Winsor’s original protocol. The observers were blinded to disease status. The spinal measurements were quantitative rather than operator-defined, taken directly from CT-imaging coordinates. The disease status — confirmed renal calculi versus controls — was established independent of the spinal measurements. The dataset began with 260 unenhanced CT scans (209 with kidney stones, 51 without); after a strict set of exclusions for osteophytes, renal masses, and other confounders that could independently affect vertebral position, 44 scans met the criteria for analysis.
The finding, published in 2025 in a PubMed-indexed osteopathic medical journal, on living patients, using twenty-first-century imaging: kidney-stone patients showed a statistically significant difference in vertebral rotation compared to controls, with the strongest association — particularly for right-sided stones — at T10, T12, and L4 (the angular rotation at those levels was the only statistically significant contributor to the difference between right-kidney-stone and stone-free scans.
In other words, a kidney stone is associated with measurable rotation of the spine at vertebral levels osteopaths mapped to the kidneys over a century ago — and a modern CT dataset showed last year.
The authors were appropriately cautious about their own work. They noted that scanner positioning is operator-dependent and could influence the measured rotations, and that the 44-scan sample may not fully account for that variability or for confounders such as psoas tightness. It is one study, on one organ system, with a modest sample and a result that suggests significance rather than overwhelming it (p = .46).
But it points in exactly the direction Winsor’s hypothesis predicts, and it does so by attempting to control the confounders his 1921 protocol lacked. The hypothesis Henry Winsor tested with cadavers is now being tested with CT imaging in living patients.
The Dissenters
Winsor has other critics, and they are not nobodies. They are the crew of skeptics that take offense to the term used in chiropractic to denote abnormal spinal structure and function (abnormal alignment and segmental motion — the kind seen in common structural pathologies of the spine), essentially denying that it has any effect on the nervous system (i.e. the vicero-somatic lesion of our discussion).
Edzard Ernst — the world's first professor of complementary medicine and arguably the most relentless academic skeptic the chiropractic profession has ever faced — has spent decades arguing that the chiropractic subluxation is a myth with no credible epidemiological evidence behind it (a drum he’s beat relentlessly both in print and on his website).
Then there’s the Science-Based Medicine crowd that gave Crislip (an internist and infectious disease specialist) his platform, singing the same song, branding the notion that spinal misalignment causes organic disease as an implausible idea not supported by any evidence. NOTE TO SELF: One wonders if the - ahem, cough-cough - ‘evidence-based’ crowd has read the most-downloaded paper their own field has ever produced — the one explaining why most published research findings are false? A fact verified by my recent two-part series on the subject (I & II). But I regress.
Watch closely what the dissenters are actually hitting, because the sleight of hand is the whole game…
They are attacking the metaphysical subluxation — Palmer's “Innate Intelligence” (see my earlier link), the multi-claim that not only do displaced vertebrae cause 95% of human disease by disrupting the nervous system, but also that the spine functions as a connection between body and soul/spirit. That is a soft target, and they are welcome to it. When I was in school in the 1980’s, the spine-as-a-bridge-to-the-Universal discussions were not only a thing of the past, they were in the distant past.
The viscerosomatic reflex, however, is a different animal entirely.
It does not require Innate Intelligence, it does not require Palmer, it does not require the word “subluxation,” or an almost-religious belief in the “33 Principles”. It requires only sympathetic segmental innervation — the documented anatomical fact that bony spurs (which are actually a downstream pathophysiological sequelae of abnormal alignment and segmental motion — a function of Wolff’s Law) physically irritate the sympathetic trunk and splanchnic nerves, mapped in cadaver studies and confirmed by twenty-first-century CT imaging.
So, pay attention to the moving cups, because one of them has the pea underneath…
One version of the chiropractic subluxation is metaphysics (what lies beyond observable nature). The other is physics (the idea that structure and function actually matter) and is found in the neuroanatomy textbooks. Collapse the two into one, and Ernst & cohort win by default. Properly separate them, and he is swinging at a scarecrow without the honest reading Winsor’s study requires.
What This Means
Henry Winsor’s 1921 study was the imperfect first observation of a real anatomical & physiological relationship. The original paper had legitimate methodological limitations — limitations that any honest reader has to acknowledge, and that any honest writer has to call out.
But those limitations have been progressively addressed by a hundred-plus years of subsequent research conducted across three independent experimental traditions: the osteopathic viscerosomatic literature beginning with Burns in 1907, the anatomical and radiographic confirmation literature running from Ussher in 1933 through Giles in 1992, and the modern imaging literature that now includes a blinded, quantitative, controlled CT study addressing the core objections to Winsor’s protocol.
The relationship between spinal alignment and visceral pathology is not folklore. It is not chiropractic marketing. It is not an artifact of one MD’s confirmation bias in a post-WWI Philadelphia dissection lab.
It is a documented anatomical relationship confirmed and re-confirmed across the span of modern medical research, and the only people who do not know this are the readers of mainstream allopathic medicine, because the institutions that train them have continued to do what the Flexner machine taught them to do — ignore what doesn’t fit the model until ignoring it is no longer possible, then rebrand it under a name that erases its history.
That rebranding is now in progress, and that is what Part 3 is about.
Part 3 — Where the Hypothesis Is Headed, and Why You Have Not Heard About It
The medical establishment that buried Henry Winsor’s study cannot bury the hypothesis itself. It can only rename it. And the renaming is well underway.
The Quiet Vindication
The frontier of twenty-first-century anatomical research has, over the past two decades, quietly arrived at a model of the human body that’s in the process of vindicating what Hippocrates, Galen, Vesalius, Willis, Still, Palmer, Burns, Korr, and Winsor were observing across two and a half millennia.
Dr. Helene Langevin (a neurologist), formerly at Harvard Medical School and now serving as Director of the National Center for Complementary and Integrative Health at the National Institutes of Health, has spent her career publishing peer-reviewed research demonstrating that the fascia — the continuous connective tissue network running through and around every muscle, organ, vessel, and nerve in the body — is not the passive packing material it was treated as for most of the twentieth century.
It is a mechanically active, neurologically innervated, biochemically responsive organ system in its own right.
Her work has documented that mechanical input at one location in the fascial network transmits along the network and produces measurable effects at distant locations, that fascial restriction alters local immune signaling and inflammatory mediators, and that the mechanical state of connective tissue is inseparable from the functional state of the organs it surrounds.
Donald Ingber, MD, PhD, at Harvard’s Wyss Institute, has spent thirty years building the mechanotransduction literature — the documented biological process by which mechanical forces applied to cells are converted into biochemical signals that alter gene expression, protein synthesis, and cellular behavior.
Mechanotransduction is now a settled field with thousands of peer-reviewed papers behind it.
To be clear, Langevin and Ingber did not set out to vindicate Palmer or Still, nor do they frame their work that way. But read their findings against the ancient hypothesis, and the convergence is hard to miss. Winsor’s premise, translated into modern language, is the textbook foundation of an entire research discipline that the medical schools now teach without ever mentioning that osteopaths, chiropractors, and a long-forgotten MD in Haverford were saying the same thing over a century ago.
The Long-COVID Vindication
The long-COVID literature has been the most dramatic recent vindication for this rediscovery, and the irony is hard to overstate. In fact, I would suggest you click every link in the following paragraph, not because you need to read every word of every study, but because the titles themselves tell the story.
Patients reporting persistent symptoms after SARS-CoV-2 infection have driven mainstream neurology and cardiology into a forced confrontation with autonomic dysfunction — dysautonomia, POTS, vagal tone disruption, sympathetic-parasympathetic imbalance — that the dominant medical paradigm spent the previous century insisting was either psychosomatic or trivial.
The published literature on post-viral autonomic dysfunction now runs to thousands of papers across major mainstream journals (link, link, link, link), and the clinical pictures being described are functionally indistinguishable from what the osteopathic viscerosomatic literature documented for decades, what the chiropractic profession has treated for over a century, and what Henry Winsor was working on in 1921.
The terminology has changed to varying degrees, but the underlying reality being described remains the same.
The spine, the autonomic chain, and the visceral organs are an integrated system; dysfunction in one produces dysfunction in the others that are on the same “electrical circuit”. And as you just saw via the work of Drs Ingber and Langevin, the medical profession is starting to once again look at patients through the lens of the model it spent a century telling the public was quackery.
And it’s telling watching how it plays out…
The Flexner machine never refuted the soma-viscera connection in 1910.
Instead, it stripped the connection from the curriculum, destroyed the schools that taught it, jailed the practitioners who applied it, and waited. Now the same principles are being rediscovered by mainstream research, but framed as “cutting-edge” twenty-first-century science rather than the vindication of a tradition as old as Western Civilization.
The Study That’s Not Being Done
What’s not happening is the study that Winsor’s hypothesis most directly demands. A study that the medical research establishment could fund tomorrow if it wanted to — Winsor Part Four: Looking Forward Through the Rear-view Mirror.
No major NIH-funded research program has ever attempted a blinded, prospective, large-cohort imaging study extending Winsor’s organ-by-organ map across the full thoracic and lumbar spine in living patients. Especially one run concurrently with a re-imagined autopsy study in the same vein as Winsor, but incorporating modern imaging techniques as well as addressing the structural shortcomings discussed earlier.
Or better yet, combine the two. The design isn’t exotic, and it isn’t hypothetical — medicine already runs exactly this kind of study, just aimed at other organs…
Researchers routinely take detailed scans of living patients, follow those patients to the end of life, and then use autopsy to confirm or falsify whether what the scan predicted actually matched the tissue — the same model used to validate brain-imaging markers against confirmed disease at death. Studies that track a group of people forward in time, measuring them at set intervals, and then recording which diseases develop in whom (Cohort Studies), are some of the oldest and best-understood tools in all of medicine.
Winsor Part Four would simply aim that proven machinery at the spine. And here are the nuts and bolts...
Enroll a large group of living patients who agree to donate their bodies to science at death — something a meaningful number of people are already willing to do when asked. Scan every spine at the start with modern imaging, measuring rotation and curvature against fixed anatomical standards, and keep the researchers doing the measuring blinded to who is sick and who isn’t — which erases the two biggest holes critics poked in the 1921 study.
Then follow the group for years and record which organ diseases show up in whom.
The anatomical map itself is not in dispute: the nerve supply to the organs leaves the spinal cord in a fixed, organ-by-organ order discussed earlier — chest organs up top, abdominal organs in the middle, pelvic organs at the bottom — settled anatomy you can find in any current reference. And because the communications running along said wiring runs both directions — a sick organ can drive its spinal segment haywire, and a bad segment can, in turn, degrade the organ it feeds — the same study captures both halves of that bi-directional loop at once.
When each participant dies, an autopsy will do exactly what Winsor did in 1921 — but now anchored to baseline imaging taken years earlier, and a written record of every disease that appeared in between. That’s the piece Winsor never had: he saw only the end state, a single snapshot with no before-picture and no timeline. Scale that across every organ he mapped — heart, lung, stomach, liver, gallbladder, pancreas, spleen, kidney, bladder, prostate, uterus — in a large group, blinded and measured, and you no longer get a 96% coincidence skeptics can wave away. You get a tested, directional, falsifiable answer.
It would take modest money, imaging equipment that already sits in every hospital, and a research team willing to publish whatever it finds (which might actually be the toughest part of the experiment — it would have to be done similarly to our elections). It would settle the question. It’s not being done.
And the reason it is not being done is the same reason Winsor’s work was buried in November 1921 and the same reason the Flexner Report was published in 1910: a body whose visceral health is governed by the structure and function of the spine is a body that does not require the volume of pharmaceutical intervention the industry’s revenue model depends on.
The economics have not changed in a hundred and four years. The question stays unanswered because the answer would be costly to industry.
Things are Changing, but the Symptom-Suppression Model Still Rules the Day
The drug-based model of modern medicine is, at its philosophical core, a model of symptom suppression rather than cause investigation (link, link, link, link, link).
Hypertension is treated with drugs that reduce blood pressure without asking why the blood pressure rose in the first place. Acid reflux is treated with proton pump inhibitors that suppress stomach acid without asking why the stomach is producing acid the body cannot handle. Migraines are treated with triptans that abort the headache without asking why the trigeminovascular system is reacting. Depression is treated with reuptake inhibitors that modify serotonin signaling without asking why serotonin signaling is dysregulated.
The chronic disease epidemic that defines twenty-first-century American health was built on this model — a model that consumes the overwhelming majority of national healthcare spending while producing the worst chronic disease outcomes of any developed nation, a fact I have documented across the evidence-based medicine archive on my old WP site.
Winsor, though, was asking a different kind of question…
He was asking what underlying anatomical relationship might explain why one tradition of healers — practitioners who used no drugs, no surgery, no hospital infrastructure, no insurance billing apparatus — was producing clinical outcomes their practitioners were willing to risk arrest to provide.
A profession whose founders adjusted patients from inside jail cells, whose practitioners were hauled into court thousands upon thousands of times by organized medicine, and whose legitimacy wasn’t secured in the final state (Louisiana) until 1974. It was not the licensed and culturally accepted profession it is today. There was no real money in it, only conviction and a burning drive to cure the masses.
The question was buried because the answer threatened too much. The answer is now being confirmed by the very establishment that buried it, in language designed to obscure the lineage.
And the lineage runs from Hippocrates to May 30, 2026, in an unbroken chain that the dominant medical tradition has spent untold amounts of time, energy, and money trying, but failing to sever.
Closing the Loop
Henry Winsor was a physician in Haverford, Pennsylvania, who published a study in 1921, confirming an ancient observation in one of the last medical journals in America that would still publish it.
The hypothesis he tested is not a chiropractic hypothesis.
It is not an osteopathic hypothesis.
It is not a homeopathic or naturopathic hypothesis.
It is arguably the oldest continuous observation in the history of Western medicine, suppressed by the institutional apparatus that had the most to lose from its acceptance, and rediscovered by doctors who could not ignore what their own observations were telling them.
The spine remembers what medicine forgot.
Henry Winsor remembered it in November of 1921. The record is still there, in a digitized archive on the open web, waiting for the next clinician, researcher, or historian willing to look.
Honored to know you Dr Jerry. Incredible! I would assume that like me, you have a respect, bordering on reverence, for what those pioneers put up with to do what we take for granted.
I've always loved the old timers - they guys that show up to meetings in suits, no matter what.
I was at a district meeting in Springfield just after starting practice, and asked one of the docs I had met how old "AJ" was because he looked really old to me. This doc told me, 'I'm not sure, but we practice in the same town, and he was here 25 years before me --- and I've been in practice 50 years.' Both passed away shortly after that.
I miss the old timers.
I grew up in Davenport Iowa, and loved going to Palmer College to get adjusted by the students. They charged one dollar, so I did it weekly. When I was a child - seventy years ago - I had a slight curvature which caused me to wear out one shoe faster than the other one. A series of adjustments over several weeks corrected it, and also cured my chronic constipation.