

What if there were a "Universal Cause" of Disease Few People Have Heard of?
The Search for Medicine's Holy Grail - The 'Common Cause' of Chronic Pain and Chronic Disease

Video and Audio Overviews
Friday, we saw one of our long-distance patients, a woman from Germany.
Her symptoms? Years of chronic, severe hip/buttock/low back pain radiating down the leg. The result of having several babies, crazy hard work, a couple major injuries, and years of military service. Although she had been dealing with it for a very long time, the pain was radically better immediately post-treatment. What was her problem? Before I answer that, let’s try to unwind what a growing number of experts are calling the leading cause of morbidity (sickness), mortality (death), pain, and dysfunction on the planet - a phenomenon known as fibrosis.
What is fibrosis, and why would I refer to it as a ‘phenomenon’? We’ll get there, but first we need to understand why fibrosis occurs in the first place. You cannot have fibrosis without inflammation. So, to understand fibrosis, you really need to first understand inflammation, realizing that there are literally thousands upon thousands of causes. Here is a list of categories; I have written about all of them at one time or another.
In medical terms, these are referred to as “insults”…

As you should notice from the infographic, inflammation and swelling are not synonymous. Inflammation is the collective name given to a group of chemical messengers your immune system makes in response to tissue-damaging ‘insults,’ allowing your cells to ‘talk’ to each other so your body can heal. In proper amounts, inflammation is a good thing; a normal, necessary, and even vital part of any and all healing processes. No inflammation, no healing. Problems, however, occur when there’s a steady supply of it hanging around for too long.
When local tissues and/or the body as a whole are continually “insulted” by repeatitive motions, poor diet (or a ‘good’ diet that ignores food sensitivities), EMF-tocicity, chronic infections, mold, chemical exposure (yes, this could be from medications), stress, old injuries that never fully heal (or heal “too much” as we’ll discuss momentarily), the inflammation becomes chronic. The body continues sending out repair signals long after the original damage is gone.
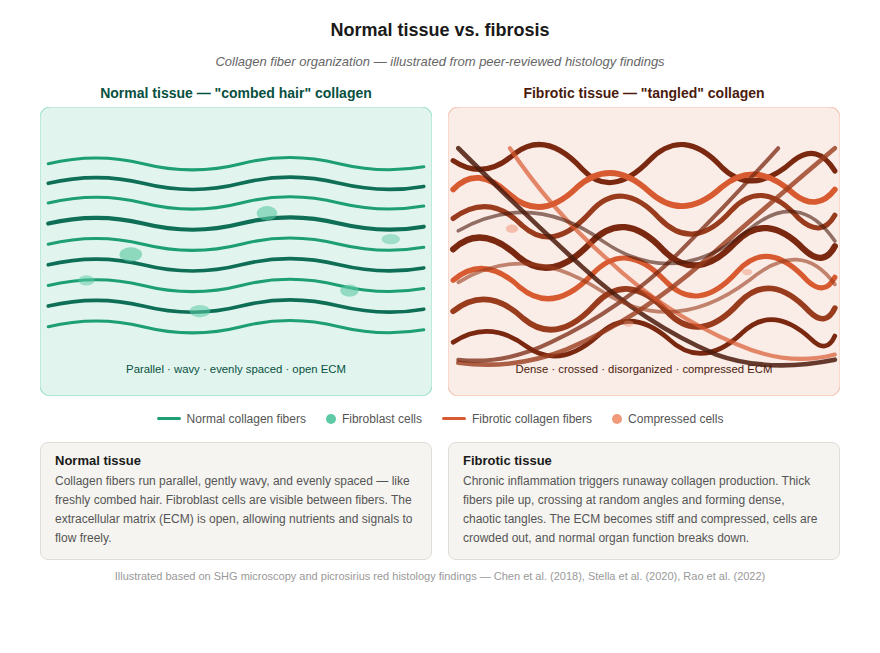
That nonstop signal is exactly what causes fibrosis to begin accumulating. It’s a cycle of dysfunction, inflammation, and fibrosis (repeat) that lays down excess collagen in a random manner, potentially turning healthy connective and muscle tissue into scar tissue. Instead of the neat, combed-hair pattern of healthy tissue, you end up with something more like a hair tangle that is stiff & inelastic, thickened & weak, and painful, even leading to peripheral nerve entrapments.
The vicious cycle starts spinning - inflammation causing fibrosis, fibrosis causing even more irritation and dysfunction, triggering still more inflammation. Breaking that cycle means dealing with both sides of the equation…
The Local Side of the Equation: Physically dealing with the scar tissue - one way or another it must be broken down for relief.
The Systemic Side of the Equation: Quieting the inflammation through diet and lifestyle (which can be a challenge, as you can see from the earlier list - a list that’s not even remotely comprehensive).
As long as the fire (inflammation) keeps raging, the scarring keeps building, with the final boot-in-the-butt being that standard imaging techniques do a poor job of showing fascia, let alone fascial adhesions. But that’s not the only reason you need to be thinking about inflammation.
Fibrosis in Organs
Fibrosis can also occur in your organs. Imagine the same processes mentioned above occurring deep inside your body, such as in your lungs, liver, heart, or kidneys. Or even your brain. The cycle keeps spinning even when it shouldn’t, and is largely the result of the same previously-mentioned insults. For instance, imagine trying to blow up a balloon made of leather. That’s kind of what pulmonary (lung) fibrosis is like.
But the concept is so much bigger than rare diseases. All of the West’s heavy-hitter killers: heart disease, cancer, diabetes, and a host of others, are considered to be diseases of inflammation and fibrosis.
Fibrosis is a pathological scarring process that leads to the destruction of organ architecture and impairment of organ function. And because inflammation always leads to fibrosis, chronic loss of organ function in most organs is associated with chronic inflammation and fibrosis (even if you are not aware it’s happening). And here’s the kicker: effective pharma-based therapies that prevent or reverse existing fibrotic lesions are not yet available (actually, there are a couple available for the above-mentioned PF, but it’s a case where the proverbial ‘cure’ is arguably worse than the disease).
Read that last sentence - the part before the parenthesis - and let it sink in, because it’s just as true today as it was in 2012, when the next study being discussed was published. And it means that despite whatever your doctor is telling you, at the end of the day, the cavalry is not coming to save you - it’s up to you. Others (friends and experts) can certainly help you along your journey, but you will have to do a significant part of the ‘heavy lifting’ on your own (I have a “Guest Post” on this topic coming soon).
Let’s take a look at one of the leading researchers on inflammation, Dr Thomas Wynn - a person trying to find the elusive ‘cure’ for fibrosis and all its ugly sequelae. Wynn is a former head of the Immunopathogenesis Section of the National Institute of Allergy and Infectious Diseases at the National Institutes of Health (the part of the NIH that Fauci ran for nearly four decades), now leading Pfizer's Inflammation & Immunology Research Unit…
Fibroproliferative diseases, including the pulmonary fibroses, systemic sclerosis, liver cirrhosis, cardiovascular disease, progressive kidney disease, and macular degeneration, are a leading cause of morbidity and mortality - nearly 45% of all deaths in the developed world - and can affect all tissues and organ systems. Fibrotic tissue remodeling can also influence cancer metastasis and accelerate chronic graft rejection in transplant recipients. Nevertheless, despite its enormous impact on human health, there are currently no approved treatments that directly target the mechanism(s) of fibrosis. -Dr Thomas Wynn from Common and Unique Mechanisms Regulate Fibrosis in Various Fibroproliferative Diseases
In another research paper, Cellular and Molecular Mechanisms of Fibrosis (175 studies in bib), Dr. Wynn goes a bit further in his explanation….
Fibrosis is defined by the overgrowth, hardening, and/or scarring of various tissues and is attributed to excess deposition of extracellular matrix components including collagen. Fibrosis is the end result of chronic inflammatory reactions induced by a variety of stimuli including persistent infections, autoimmune reactions, allergic responses, chemical insults, radiation, and tissue injury.
ECM? Most of you have at least an idea of what collagen is, but what is the ECM (extracellular matrix), and what is its job? That question is answered by yet another scientific article (The Extracellular Matrix at a Glance) published in the Journal of Cell Science (quote is cherry-picked for time and space constraints).
The extracellular matrix (ECM) is the non-cellular component present within all tissues and organs, and provides not only essential physical scaffolding for the cellular constituents but also initiates crucial biochemical and biomechanical cues. Although, fundamentally, the ECM is composed of water, proteins and polysaccharides [long chains of sugar molecules], each tissue has an ECM with a unique composition and topology.
Moreover, the ECM is a highly dynamic structure that is constantly being remodeled. Through these physical and biochemical characteristics the ECM generates the biochemical and mechanical properties of each organ, such as its tensile and compressive strength and elasticity, and also mediates protection by a buffering action that maintains extracellular homeostasis and water retention.
Acute injury activates the fibrogenic machinery and induces wound healing. In a healthy tissue, once the wound has been repopulated [with collagen and ECM], strict feedback mechanisms are initiated that ensure restoration of tissue. Under extreme conditions, such as repeated injury, these aberrant conditions promote chronic vascular remodeling and enhanced ECM crosslinking that eventually leads to aberrant fibrosis and an inability of the tissue to heal properly.
This aberrant wound healing scenario is characterized by the altered mechanical stability and reduced elasticity that is typical of scarred tissue. In extreme cases, a chronic wound can also promote a tumor.”
Did you catch that….?
Scar Tissue (fibrosis) not only leads to chronic pain, but to sickness, disease, and death, doing so by creating a microscopically “crosslinked” hairball-like web or net of aberrant collagen and ECM (see earlier image).
This web not only causes mechanical restriction, but thickened fascia is weak, as well as hypoxic, with the tangle effectively choking off blood supply via enmeshing and then strangling the capillary beds, which causes low O2 levels and pain, as well as an impaired ability to heal. The important thing to remember is that this process can occur anywhere in your body, including organs.
In his NIH bio, Wynn nibbled around the edges by revealing that said “injuries” can occur in a variety of ways. “Fibrotic tissue remodeling is the final common pathological outcome of many chronic inflammatory and infectious diseases.” In his paper, he spelled it out. “Fibrosis is the end result of chronic inflammatory reactions induced by a variety of stimuli, including persistent infections, autoimmune reactions, allergic responses, chemical insults, radiation, and tissue injury“. I think you will find all of those on the previous list.
Of these, the easiest to control is the “chemical insults“. Huh? The truth is, the average American is chemically insulting their body on an almost hourly basis via the garbage we continue shoving into our collective pie holes. But I regress…
Fascial Adhesions & Proprioceptive Dysfunction as the Common Cause of Disease?
“Connective tissue is something of an orphan child in medicine: although it is an integral part of the musculoskeletal system, connective tissue is basically absent from orthopedic textbooks, which deal principally with bones, cartilage, and muscles. Nonspecialized connective tissues, which form what’s known as the fasciae and envelop all muscles, nerves, bones, and blood vessels, are typically allotted a short paragraph in current textbooks, if mentioned at all.
And despite increasing evidence of its role in chronic pain and other diseases, connective tissue is not very well studied. In contrast to the general neglect of connective tissue in the conventional medical and scientific fields, “alternative-medicine” researchers, and especially clinical practitioners, have for many years recognized the potential importance of connective tissue in health and disease.
Indeed, a variety of alternative manual and movement-based therapies work under the collective assumption that connective-tissue pathology lies at the source of musculoskeletal pain, and that this can be ameliorated with manual treatments.” Some cherry-picked sentences from Dr. Helene Langevin’s article, The Science of the Stretch from the May 2013 issue of The Scientist journal
Although I do not believe there is a “one cause, one cure” for all pain, sickness, and disease (except this), it would behoove us to pay attention to research that’s been circulating in the academic medical community for decades. This research concerns something that mankind has been searching for for thousands of years — medicine’s Holy Grail, if you will — the ever-elusive “Common Cause” of pain, sickness, and even death (think ‘transhumanism’ in 2026)
Is this search for a Universal Cause of sickness and disease a pipe dream, or could there be solutions that the mainstream (namely, big pharma) continues hiding? Or at least hiding until someone Wynns wins the race for the Holy Grail in the form of a blockbuster drug - a drug that will likely be the subject of lawyer ads within a few years of release, but make mountains of cash in the meantime? You’ll know when it happens - just watch for the commercials!
Although tendons, ligaments, and others are important, when you think of connective tissues, think fascia. Once you start to understand a little bit about how the body functions, it is not a reach to grasp how big a part Fascial Adhesions play, not only in the development of Chronic Pain Syndromes, but in the development of various disease processes as well.
Over a century ago, two pioneers in the field of natural medicine, B.J. Palmer (chiropractic) and A.T. Still (osteopathy), developed healing philosophies and systems based on their belief that there was a Common Cause of all disease. And although they did not agree on what this common cause was, they may have both been closer to the truth than anyone could have known at the time.
The former thought that this “Common Cause” was nerve interference caused by misaligned or malfunctioning vertebrae, while the latter believed that disease was largely the result of restrictions or adhesions of the fascia. It seems that medical research may be proving both of them correct. Enter Drs. Donald Ingber and Helene Langevin.
Donald Ingber & Helene Langevin: Fascia’s Role in Chronic Pain, Chronic Illness, and Death
After earning her MD degree in 1978, Dr. Helene Langevin did post-doctoral work in Neurochemistry at Cambridge in England before doing her residency in Internal Medicine and fellowship in Endocrinology and Metabolism, both at Johns Hopkins. In 2018, she was appointed Director of the National Center for Complementary and Integrative Health (NCCIH) at the National Institutes of Health, a position she held through the end of 2023, meaning that for over five years, the federal agency overseeing all integrative medicine research in the United States was being run by a fascia researcher. She remains a professor at Harvard Medical School.
Some of her chief areas of study include the relationship of lower back pain to fascia, as well as acupuncture to fascia. She was also part of the you-need-to-see-it-to-believe-it study that imaged adhesed fascia in motion, comparing it, side-by-side to normal fascia in ten-second videos (the topic of my next post).
Dr. Ingber is no ordinary cell biologist. He's also a medical doctor with advanced degrees in molecular biophysics and cellular biochemistry (all from Yale). Since 2009, he's been the Founding Director of the Wyss Institute for Biologically Inspired Engineering at Harvard, the Judah Folkman Professor of Vascular Biology at Harvard Medical School and Boston Children's Hospital, and Professor of Bioengineering at the Harvard School of Engineering and Applied Sciences.
Ingber has published over 500 research papers in peer-reviewed scientific / medical journals, and his bio states that “Ingber’s insights have helped create the fields of mechanobiology, angiogenesis, tissue engineering, nanobiotechnology, and biomimetics”. He is also the inventor of “human-organ-on-a-chip” technology, which is replacing animal testing models, and was recognized by the National Academy of Engineering.
In the amazing 2003 study published in the ‘Annals of Medicine’ titled Mechanobiology and Diseases of Mechanotransduction, Dr. Ingber shed new light on an old topic — the search for the “Common Cause” of sickness and disease. Although Dr. Ingber himself would never tout his research as a quest to find medicine’s “Holy Grail,” he certainly believes that the basis for the largest percentage of today’s diseases is directly related to dysfunctional mechanoreception / proprioception of connective tissues.
We already know what connective tissues are, but what in the world is proprioception / mechanoreception, and how does it relate to health?
The word ‘proprioception’ (aka mechanoreception) comes from two words. First is the Latin word ‘proprius,’ meaning “one’s own”. The second is the word ‘perception’, meaning the process by which one translates sensory input into a coherent and unified picture of one’s environment. Thus, proprioception is the sense or “perception” of the relative position of various parts of the body in relationship to their environment.
In other words, proprioception is your body’s ability to unconsciously know where its various body parts are in space as well as how they are moving in relationship to each other at all times and in all circumstances. Where is the heaviest density of mechanoreceptors found? Fascia, of course!
It is this internal sense of proprioception that tells you whether your body (or a part of your body — i.e. a limb) is moving, how fast it is moving, what direction its moving, and how much energy is being expended to move it; as well as where the various parts of the body are located in space — in relation to every other part of the body.
Incredible proprioceptive ability is one of the factors that make a great athlete, a great athlete. Watch some old highlights of a couple of Kansans, Darren Sproles or Barry Sanders, to see what I mean! As you start to grasp how complex and vital proprioception is, you can begin to understand why it has been said that it is more important than the inner ear for balance.
When proprioceptive nerve endings (mechanoreceptors) are stimulated via stretch, movement, or pressure, the nerve input is fed to the brain via the spinal cord and nerve system. Once in the brain (cerebellum), these impulses are decoded, translated, and integrated into something the body can understand. Messages are then created and sent out to the various parts of your body as responses. There is a continual feedback loop, with the whole process taking mere microseconds to accomplish. When it all works perfectly, it’s literally poetry in motion.
But when it doesn’t work perfectly…
When this system begins to break down, all sorts of problems can arise — many of them ugly, severe, and as you’ll soon see, not well understood by a medical community that, since the Flexner Report, has been trained to think of a drugs & surgery first approach to treatment. What are the most common ways that this system goes haywire? Let’s talk about it in terms of the bi-directional model laid out by Drs. Palmer and Still, 100+ years ago, and discussed above.
Firstly, abnormal biomechanics, whether skeletal or fascia, lead to both inflammation and fouled-up proprioception, which together cause degeneration of the affected joint(s). This is not controversial and can be found in any pathology textbook. The scientific literature is clear — loss of normal joint motion causes a loss of proprioception that leads to joint degeneration, and this degeneration turns right around and causes more abnormal motion and proprioceptive loss. Ladies and gentlemen, start your cycles - your vicious cycles! A causes B, and B causes A — with the whole thing churning out a steady stream of inflammation. It’s a recipe for disaster.
Secondly, using this model, let’s think about what loss of joint motion and the subsequent loss of proprioceptive input could theoretically do to the various organs and organ systems in the body. Because the brain ultimately controls every function of the body via the spinal cord and nerve system, a loss of range of motion and proprioception has actually been shown to diminish organic (organ) function. Sound crazy? Not to B.J. Palmer. Not to A.T. Still. And not to Doctors Ingber or Langevin either.
It is a simple physiological fact that loss of spinal range of motion due either to vertebral subluxation (loss of alignment or movement) and/or Fascial Adhesion causes diminished nerve system (proprioceptive) function. Amazingly enough, this loss of mechanoreception turns around and causes a loss of motor nerve function. The real stunner, though, is that recent scientific research has shown us exactly how this occurs!
In a lecture I attended over three decades ago by the venerable Dan Murphy, he showed research (probably this) saying that in healthy people, for every proprioceptive impulse (sensory – afferent) that is fired up to the brain, there are approximately 30 return nerve impulses (motor – efferent) coming back down in response. This is the basis of one of the singularly wildest studies in American history - Sympathetic Segmental Disturbances—II. The Evidences of the Association, in Dissected Cadavers, of Visceral Disease with Vertebral Deformities of the Same Sympathetic Segments (aka, “The Winsor Autopsies”) - published in a 1921 issue of the Medical Times.
It is the body’s motor impulses that tell it what to do and how to function - tells my fingers how to type, tells my heart how and when to beat, tells my intestines to work in tandem with my stomach, colon, pancreas, liver, etc, and tells my immune system to attack or not attack, depending on the threat. Oh, I may have forgotten to mention it, but fascia also happens to be the single biggest proprioceptive organ in your body.
The Vercerosomatic Lesion as Related to Fascia
Going back to the earlier-mentioned study, every time a proprioceptive nerve ending is not being stimulated like it should be (usually due to restricted range of motion of a particular joint), 30 returning motor responses from the brain to the body are being inhibited. In other words, loss of spinal range of motion causes a corresponding loss of proprioception, affecting motor nerves at an astounding 30:1 ratio.
This then affects not only the way muscles and joints function, but also the way that organs function. Whoa! Sounds like both Dr. Still and Dr. Palmer may have been way ahead of their time! And although these men have frequently been labeled by the mainstream medical community as quacks, this concept of the “Vicerosomatic Lesion” has been in the scientific medical literature since the early 1900’s.
Although it’s a three-dollar doctor word, “vicerosomatic” simply means that dysfunctioning areas of the spine or body (the soma) can present with palpable, localized, and sensitive symptoms directly related to corresponding visceral (organ) dysfunction (see the Winsor Autopsies study). And the interesting thing is that the dysfunction cuts both ways. Problems in the viscera can cause problems in the soma, or problems in the soma can cause problems in the viscera. It’s a two-way street — an open phone line of communication, if you will. Or at least it should be.
The beauty of chiropractic adjustments coupled with scar tissue remodeling is that they not only help relieve pain while restoring range of motion, they actually allow the nerve system and the various functions controlled by the nerve system (basically everything in the body, including organs) to function closer to the way they were designed and created to function in the first place. Doubly cool is that once you start addressing the “tethering effects” of the microscopic fibrosis I usually refer to as scar tissue with my patients, you won’t feel like you constantly need to be adjusted.
BACK TO DR. INGBER
Dr. Ingber believes that modern medicine is far too wrapped up in trying to pin all our health problems on genetics, while mostly ignoring what he believes to be the greatest underlying causes of disease. What are these underlying causes of disease he speaks of? His research in biophysics and pathology has led him to the conclusion that many, if not most, of the problems people seek medical care for are the result of abnormal structure and function of the body’s connective tissues (bones, ligaments, tendons, fascia, etc).
Furthermore, he believes that you cannot truly understand any disease process without first understanding biomechanics and cell biology — the relationship between how the body functions mechanically, and proper cellular function (which is itself, almost incomprehensibly complex).
Remember his article, Mechanobiology and Diseases of Mechanotransduction that we mentioned earlier? “Mechanotransduction” is defined by Dr. Ingber as the method by which cells both sense and respond to mechanical stresses. In a subtle slap to the face of his own profession, while inadvertently validating what chiropractors and ye olde osteopaths have been saying for well over a century, he notes that numerous diseases from across the entire spectrum of medical practice share a common cause.
In his article, Dr. Ingber states this about sickness and disease: “their etiology [cause] or clinical presentation [symptoms] results from abnormal mechanotransduction”. In other words, a brilliant medical doctor from Harvard is saying that, at the very least, a significant amount of sickness and disease are being caused by loss of proprioception, and the subsequent abnormal neurological activation patterns that follow (check out this conversation I had about mechanotransduction with one of the strongest men on the planet).
Here are some of the points (quotes) from Dr. Ingber in his ground-breaking paper — a paper that was published long enough ago that more professionals should be aware of its paradigm-exploding implications.
Mechanical forces are critical regulators of cellular biochemistry.
There is a huge disconnect between ‘genome-age’ technologies and the reality of how diseases manifest themselves. From the time the first human looked, listened and felt for what is wrong with a sick friend, caregivers have recognized the undeniable physical basis of disease.
In the current genome euphoria, there appears to be no place for ‘physicality’. This is especially worrisome given that abnormal cell and tissue responses to mechanical stress contribute to the etiology and clinical presentation of many important diseases, including asthma, osteoporosis, atherosclerosis, diabetes, stroke and heart failure.
There is strong mechanical basis for many generalized medical disabilities, such as lower back pain and irritable bowel syndrome, which are responsible for a major share of healthcare costs world-wide.
In biology and medicine, we tend to focus on the importance of genes and chemical factors for control of tissue physiology and the development of disease, whereas we commonly ignore physical factors. This is interesting because it was common knowledge at the turn of the last century that mechanical forces are critical regulators in biology.
These new insights into mechanobiology suggest that many ostensibly unrelated diseases may share a common dependence on abnormal mechanotransduction for their development or clinical presentation.
Understanding of the relation between structure and function in living tissues and of fundamental mechanisms of cellular mechanotransduction may therefore lead to entirely new modes of therapeutic intervention.
And although some level of medical prejudice might be what prevented him from adding the words “chiropractic” or “chiropractic adjustments” to the following list, he essentially validated the profession by stating, the therapeutic value of PT, massage, and muscle stimulation is also well known.
Dr. Ingber went as far as saying…
“Moreover, most of the clinical problems that bring a patient to the doctor’s office result from changes in tissue structure and mechanics. Although these physical alterations have been commonly viewed as the end-result of the disease process, recent advances in mechanobiology suggest that abnormal cell and tissue responses to mechanical stress may actively contribute to the development of many diseases and ailments. Thus, it might be wise to search for a physical cause when chemical or molecular forms of investigation do not suffice.”
If you do not grasp how big this concept being promoted by Dr. Ingber really is, re-read the quote until you do. Especially those of you who have been through every conceivable medical test under the sun in a fruitless quest to figure out what is wrong with you!
This is No Longer a Two-Person Conversation
Not that long ago, Drs. Ingber and Langevin were essentially the lone medical voices (at least with this level of clout) saying these things publicly. That’s no longer the case. Over the last decade or more, an entire international research community has formed around fascia, connective tissue, and mechanotransduction, and several of these names are worth knowing.
Dr. Carla Stecco, an orthopedic surgeon and Professor of Human Anatomy at the University of Padua in Italy, has done over a hundred unembalmed cadaver dissections and her 2015 textbook, Functional Atlas of the Human Fascial System, is now the reference for anyone serious about fascial anatomy. She and her brother, Antonio (also an MD), co-authored the paper that put the term “densification” on the map — Painful Connections: Densification Versus Fibrosis of Fascia — which directly ties pathological changes in fascia to chronic pain syndromes that mainstream medicine still can’t explain.
Dr. Robert Schleip, who heads the Fascia Research Group at the University of Ulm and Technical University of Munich in Germany, won the Vladimir Janda Award for his work showing that fascia isn’t just passive packing material — it actually contracts on its own, like smooth muscle. His foundational paper, Active Fascial Contractility, helped kick off the modern fascia research movement, and his 2019 follow-up, Active Contractile Properties of Fascia, shows how myofibroblasts inside the fascia drive the same kind of pathological contractures we see in chronic pain patients. Schleip co-organized the first Fascia Research Congress at Harvard Medical School in 2007 and has been at every one since.
Dr. Yuval Rinkevich is the newer name and arguably the most exciting. His 2023 paper in Nature, CD201+ Fascia Progenitors Choreograph Injury Repair, reframed fascia as an “active donor tissue” — meaning fascia cells actually migrate as pre-assembled patches into wounds and drive outcomes; whether you heal cleanly or with fibrosis/scar. His 2024 follow-up in the American Journal of Physiology, Organ Dependency on Fascia Connective Tissue, goes a step further and explicitly argues that the fascia system regulates pain sensation, organ inflammation, trauma response, and fibrotic disease throughout the body.
Others: There are too many others to count, including Thomas Findley (Rutgers / NJ Medical School — co-founder of the Fascia Research Congress, fascia and oncology), Peter Huijing (Vrije Universiteit Amsterdam — myofascial force transmission, intermuscular connections), Andry Vleeming (University of New England / Ghent — sacroiliac joint, thoracolumbar fascia anatomy, force closure model), Frank Willard (University of New England — thoracolumbar fascia neuroanatomy, foundational anatomy chapters), Jaap VanderWal (Maastricht University, Netherlands — embryology and architecture of fascia, "the architecture of the connective tissue"), Bruno Bordoni (Foundation Don Carlo Gnocchi, Milan — fascia, breathing, and chronic pain interconnections), Mary Cowman (NYU — hyaluronan biochemistry, frequent Stecco collaborator), Rebecca Pratt (Oakland University / William Beaumont School of Medicine — "Hyaluronan and the Fascial Frontier," densification physiology), Paolo Tozzi (Italy — osteopathic fascia research, fluid dynamics of fascia), Leon Chaitow (deceased 2018, but worth listing — UK-based, prolific author and editor of Journal of Bodywork and Movement Therapies, helped legitimize fascia in manual medicine), Werner Klingler (Ulm — fascial contractility and smooth muscle-like behavior, Schleip collaborator), Jan Wilke (Goethe University Frankfurt — myofascial chains, remote stretching effects), Stephen Levin (independent researcher — biotensegrity, mechanical model of the body that bridges Ingber's cellular work to the macroscopic musculoskeletal system). My apologies because I know I left out many...
What Does it All Mean?
In the famous words of Arnold Schwarzenegger’s character, Dutch, from 1987’s hit movie, Predator, “If it bleeds, we can kill it.” The first part of solving these sorts of problems is figuring out what the heck might be causing them in the first place. Sorry, but simply covering symptoms is no longer an option (my article on what it takes to Restore Proprioceptive Integrity in Fascia).
It also means that while their model was far from factually accurate (hard bones pinching soft nerves - while physiologically incorrect, it is functionally accurate), chiropractors, in many respects, have been light years ahead of standard drug therapy, simply because historically, they’ve understood the benefits of their adjustments. But chiros are no longer the lone voice crying out in the wilderness.
The type of advanced research being done by a growing number of elite researchers is certain to attract a host of brilliant doctors, scientists, engineers, and scholars who are likewise interested in finding the “Common Cause”. And while the Osteopathic profession has largely given up on this concept in order to become R.D.’s (”Real Doctors”), the chiropractic profession (at least geezers like me) still largely embraces “The Big Idea” as espoused in its various forms by men like Palmer, Still, Ingber, Langevin, and others.
Unfortunately, when you are bucking “The System,” the process can be a long, slow, uphill battle. No, the word “battle” was not a mistake. In fact, I probably should have used the word “war”. But anything worth having is worth fighting for. In the words of Theodore Roosevelt, “Nothing worth having comes easy”.
Now, back to the question I asked in the opening paragraph….
What was her (the patient from Germany) problem? She had severe fascial adhesions in her low back and upper buttock (women will always call this their hip), wrapping around to her hip flexor and halfway down her quad. The result was exactly what you might expect to see after reading this post.
If you stay tuned for my next post, I am going to dig into one of the most wacky facts in the world of orthopedics - something that not one person in a thousand is aware of. The majority of back pain falls into a category known as “Nonspecific”. Contemplate what that really means, and until next time, God bless!
Nice Rob. You are correct about the drugs (which I mention as a form of toxicity / inflammation). You are also correct that anti-inflammatories cause incomplete and abnormal healing - that information has been around for probably three decades or more. I also recommend rebounding as a form of lymphatic pumping - I left a link for it somewhere, but here it is again, https://doctorschierling.com/blog/the-health-benefits-of-bouncing-on-a-trampoline. Honestly, there are lots of ways, thanks for sharing!
A lot of factors lead to this tangled mess of fibers.
Anti inflammatories and pain killers hinder the body's ability to finish the repair job.
Also, the lymph system relies on movement in order to clear debris. If lymph is stagnant, repairs are sub optimal.
This channel on YouTube helped me a lot. Here's a video on how to get the lymph fluid moving along with simple exercise in order to regain range of motion.
https://youtube.com/watch?v=Bn4RX0UbEhY
Some of my old injuries flared up and after the re-repair they have been much better. I also recommend QiGong which is another great way to exercise and get the body to loosen up tight fascia.