

What if You Could Visualize Your Chronic Back Pain?
When it Comes to Your Pain, Seeing is Believing

Audio and Video Overviews
Chapter 1: The Revelation
In one of my radiography classes, taught by renowned radiologist Norman Kettner, he put up a lateral neck X-ray on the overhead projector (yes, this was, after all, the 1980’s) and asked the class, “What’s wrong with this person?” After a while, people were making ridiculous guesses - rare diseases for which there were fewer than 100 known cases in history.
After about five minutes of this, he told the class what was wrong with the person. They were dead. It seems that the university took X-rays of all the cadavers received by the anatomy lab - for research purposes. And although as I remember, the film itself was rather clean (no remarkable findings), that lesson stuck with me. Fast forward twenty-plus years…
After taking lots of X-rays the first two decades of practice, 15 years ago, I completely quit, getting rid of my equipment - one of the single best decisions I ever made. For years, I had been becoming increasingly disillusioned, coming to the realization that X-rays were not only largely unhelpful for what I was doing in my clinic, but that I could not, in any consistent and tangible way, correlate them to my patients’ symptoms.
I was not the only person coming to this conclusion…..
Chapter 2: The Studies
Right around that time, there was an explosion of studies on this topic, of which there are now hundreds. The theme of these studies is that correlating imaging to back pain is not only difficult, it’s extremely difficult. Let’s look at a few of the important ones, chronologically.
The study that kicked everything off took place while I was still in school (1990), when the Journal of Bone and Joint Surgery published Abnormal MRI Scans of the Lumbar Spine in Asymptomatic Subjects: A Prospective Investigation. The authors imaged 67 people who had never had low back pain, sciatica, or neurological symptoms, finding substantial abnormalities in roughly one-third. Among those under 60, 20% had a herniated disc. In the over-60 group, 57% had abnormal scans, including 36% with disc herniation and 21% with spinal stenosis (a shrinking of the spinal canal).
Next came the study that started (emphasis on ‘started’) changing guidelines - 1994’s Magnetic Resonance Imaging of the Lumbar Spine in People without Back Pain that was published in the NEJM. This study looked at just under 100 individuals with no history of back pain or problems, with the authors coming to the realization that a great number of individuals with no history of back pain had disc bulges, underscoring the difficulty of establishing imaging findings as the source of pain.
On MRI examination of the lumbar spine, many people without back pain have disk bulges or protrusions... Given the high prevalence of these findings and of back pain, the discovery by MRI of bulges or protrusions in people with low back pain may frequently be coincidental.
Then, in 2001, the authors of the first study above did their Seven-Year Follow-Up, which was actually an 11-year follow-up study in which subjects reported on back pain development over a seven-year recall period. The researchers tracked the original 67 asymptomatic subjects for seven years, learning that the findings on their original MRI scans were not predictive of the development or duration of low back pain. Individuals with the longest duration of low back pain did not have correspondingly worse imaging findings at baseline. In other words, the scan you get today will not necessarily tell you much about tomorrow.
The findings on magnetic resonance scans were not predictive of the development or duration of low-back pain. Individuals with the longest duration of low-back pain did not have the greatest degree of anatomical abnormality on the original, 1989 scans.
Next, in 2006, came the cleverest of the studies (Are first-time episodes of serious LBP associated with new MRI findings?). Dr Carragee's Stanford team scanned 200 people at baseline - before any significant back pain - then rescanned them after a serious LBP episode developed. They found that findings on MRI within 12 weeks of serious LBP onset were highly unlikely to represent any new structural change. Most ‘new’ findings (loss of disc height, facet degeneration, endplate changes) represent age-related changes that accumulate silently. In other words, clinicians were routinely attributing pre-existing findings to the acute episode.
Eight years later, in 2014, a Washington State University study (“LAIDBACK”) came to similar conclusions. Over a three-year period, the authors watched people develop new MRI findings, asking whether those new findings caused new symptoms. The take-home was that only a handful of very specific findings showed any meaningful link, and even those were rare enough to leave most LBP unexplained by imaging.
Even when applying more specific definitions for spine-related symptom outcomes, few MRI findings showed large magnitude associations with symptom outcomes. Although incident annular fissures, disc extrusions, and nerve root impingement were associated with incident symptom outcomes, the 3-year incidence of these MRI findings was extremely low, and did not explain the vast majority of incident symptom cases.
In 2015 (Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations), a group of researchers reviewed 33 high-quality studies, covering 3,110 asymptomatic individuals (people without symptoms or pain), discovering that disc degeneration was present in 37% of pain-free 20-year-olds and 96% of pain-free 80-year-olds, with disc bulges, protrusions, and annular fissures (cracks in the disc) showing similar age-related prevalence in people who had no pain at all.
Imaging findings of spine degeneration are present in high proportions of asymptomatic individuals, increasing with age. Many imaging-based degenerative features are likely part of normal aging and unassociated with pain. These imaging findings must be interpreted in the context of the patient's clinical condition.
The 2023 update of 2014’s Steffens’ Review included about three times as many studies as the original. The update found that in populations with current LBP, Modic type-1 changes and disc degeneration showed weak associations with worse pain or disability outcomes, while disc thinning (height reduction), disc herniation, spinal stenosis, and others showed no evidence of association with long-term clinical outcomes. In other words, the overall picture remained the same - profound disconnect between scan and symptom.
The results suggest that some MRI findings [the two mentioned above] may have weak associations with future LBP…
Last year, the 2025 PRISMA-compliant systematic review team analyzed data from 1,247 patients across 45 international centers, examining the correlation between lumbar MRI findings and chronic low back pain (Correlation Between Clinical and Imaging Findings in Lumbar Magnetic Resonance in Patients with Chronic Low Back Pain: A Systematic Analysis). Its chief finding?
Radiological findings such as disc herniations or disc degeneration are present in up to 93% of asymptomatic individuals over 60, raising serious questions about their clinical relevance. The takeaway is simple: what radiologists flag as abnormal in older spines is largely a normal feature of aging with no reliable relationship to who is actually in pain.
The correlation between lumbar MRI findings and LBP is considered moderate to weak in a large percentage of cases, due to the high prevalence of abnormalities in asymptomatic individuals and the influence of non-anatomical factors… This means that even if abnormalities are visible on the imaging, they do not always translate into a clear diagnosis or the cause of the patient’s pain.
I could have gone on and on, but the point of this chapter is simple. Consensus among nearly all these reviews is some version of: “These imaging findings must be interpreted in the context of the patient’s clinical condition,” which is the polite scientific way of saying that imaging on its own doesn’t tell you who hurts today or predict who will hurt tomorrow.
Chapter 3: The Culprit
What if you learned that the number one type of back pain on the planet - by far - is actually called “Non-Specific Low Back Pain” or NSLBP/NSBP? Any idea what that really means? It’s yet another example of the gap chasm/canyon between academic medicine and clinical practice. And it begs an important question: If non-specific back pain is the #1 type of back pain, what the heck is causing it?
For decades, researchers assumed back pain had a straightforward explanation; bad discs, weak muscles, or poor posture. As you should have started to notice from the previous chapter, that model has largely collapsed. Again I ask you; what the heck is causing all that pain?
Although theories abound, when I asked Claude (AI) how many studies there are on Non-Specific Back Pain, its answer was…
The total is likely in the 50,000–80,000 range, and well over 100,000 if you include studies where NSLBP is a significant secondary focus. What makes this particularly striking is the punchline: despite being arguably the most studied pain condition in human history, we still cannot reliably identify a structural cause in 85–95% of cases. That’s not a gap in the research — that’s the research telling us something profound about where we’ve been looking. Or not looking.
When you start down the chronic Non-Specific Back Pain rabbit hole (and trust me, it’s a verifiable rabbit hole), you’ll come across a host of topics I’ve written about in the past, including Central Sensitization. But before we tackle CS, let’s look at the factor that the majority of experts believe is causing most chronic NSLBP - psychosocial factors.
In the scientific literature, these would include fear-avoidance beliefs / catastrophizing, depression, anxiety, and others. In other words, patients who believe their spine is damaged beyond repair and that movement is dangerous will guard and restrict movement, creating a self-reinforcing pain cycle which, as we saw from earlier studies, often has nothing to do with their imaging or what’s really wrong with them.
Next we have “Central Sensitization”. CS is a neurological phenomenon where people end up with altered nociception (the brain senses pain in the absence of visible tissue damage - pay attention to the word “visible” because it is critical to where we are headed), and where one’s nervous system essentially “learns” pain. In this group, the pain responses become pathologically amplified, leading people to experience pain that’s disproportionate to any identifiable physical cause.
I’m going to piss some people off here, but I think that in far too many cases, these two concepts (psychosocial factors & Central Sensitization - arguably the biggest in the NSLBP world) get more credit than they’re actually due. For instance, my experience tells me that far more people are depressed or anxious because of their pain, not the other way around (I would love to hear people’s opinion of this in the comment section).
After 35 years of practice, and working extensively with fascia since ‘99 or 2000, I’ve come to believe that fascial adhesions - particularly in the thoracolumbar fascia (the diamond-shaped area of white tissue in the lower back) - is arguably the biggest cause of NSBP. Let’s see why I might think that…
The Thoracolumbar Fascia
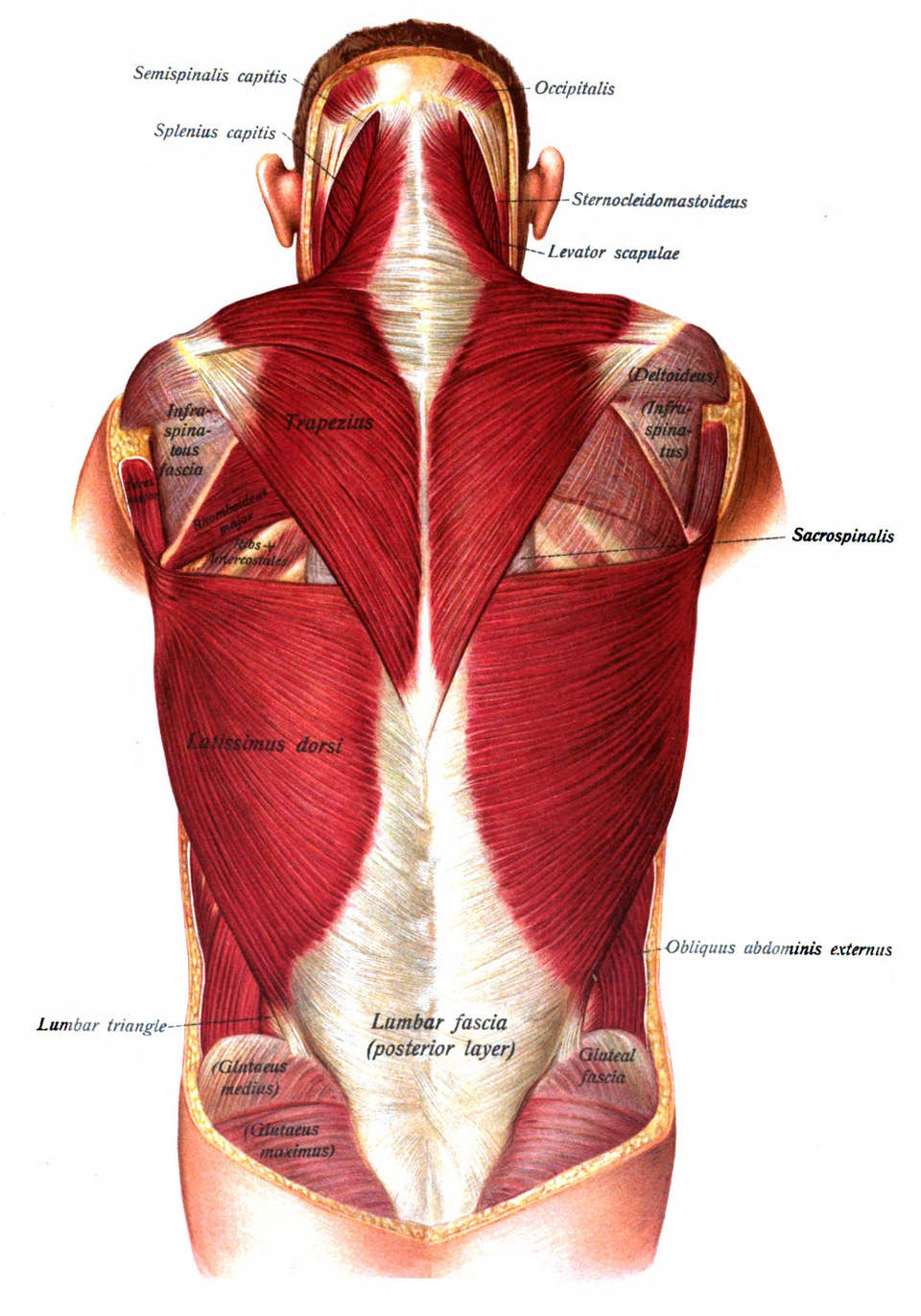
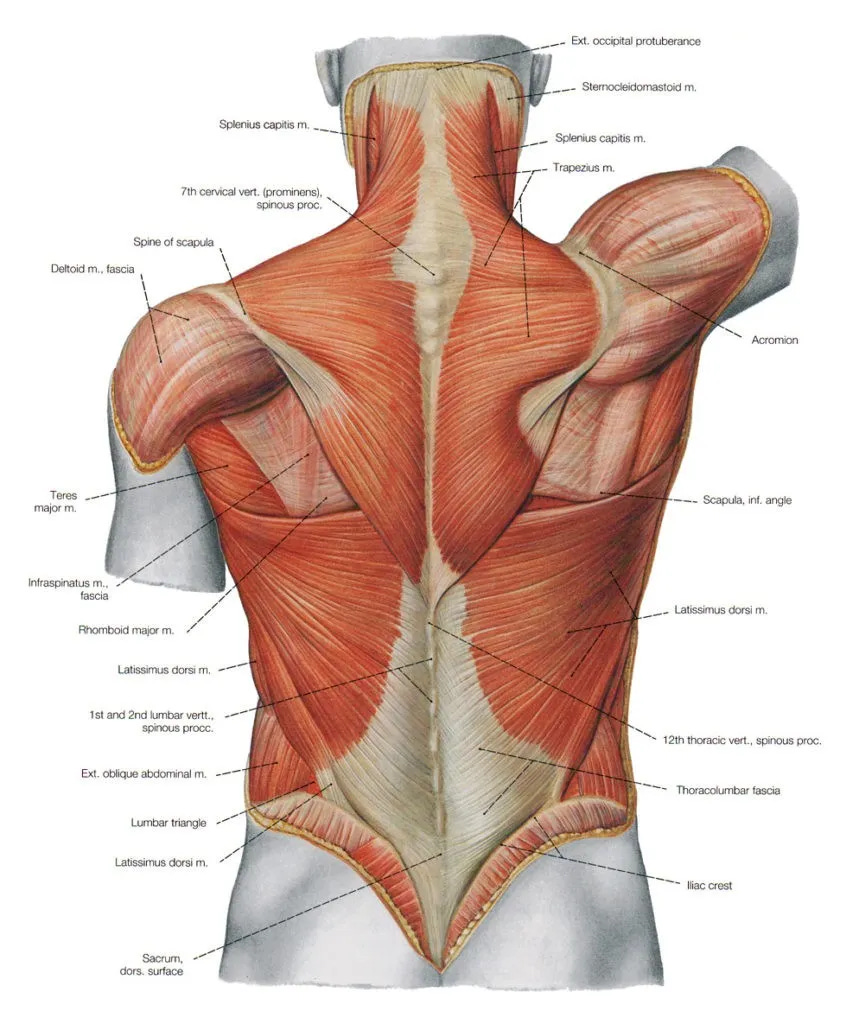
The thoracolumbar fascia has three distinct layers made up of muscle tendons (which are basically made up of the same “stuff” as fascia) and is important for both trunk stability and load transfer, which is why it continually appears in discussions of mechanisms of LBP and core rehab (see my post on Lower Crossed Syndrome for more information).
What if, instead of being ‘either-or’ as far as fascial adhesions or Central Sensitization, it was potentially both (‘and’) - at least in some of the more severe cases? What percentage of the cases? No idea. However, a recent hypothesis connecting Central Sensitization directly to the fascia got my attention.
Researchers have shown that chronic pain signals can trigger a chemical reaction in the body's connective tissue, releasing inflammatory substances, in a process coined ‘neurogenic inflammation’ (2023 study, 2025 study). This process causes the fascia - the thin, slippery wrap surrounding your muscles - to thicken, stiffen, and ‘tether’ normal motion in a process increasingly referred to in the peer-reviewed literature as “densification” (you will see examples in the “Videos” chapter).
Think of it like lubricated plastic wrap that slowly turns into dry, crusty duct tape. As you might imagine, this fascial thickening impairs the smooth gliding between muscle layers, irritates nearby nerve endings, and traps inflammatory fluid in the tissue, creating a self-sustaining cycle of pain and stiffness that can persist long after the original injury has healed.
Moving forward…
Remember Dr Helene Langevin from my last post - the brilliant neurologist who is interested in both acupuncture and fascia, and thinks that biomechanical dysfunction is the cause of the vast majority of chronic pain and chronic illness?
This entire concept of thoracolumbar fascial adhesions / densification is exactly what Langevin’s famous 2011 ultrasound study captured. Shear strain between the layers of the thoracolumbar fascia of individuals with chronic LBP was dramatically different from that of healthy controls (those without chronic LBP). Pay attention because in many cases, low back pain can actually be visualized…
Chapter 4: The Videos
The 2011 Langevin paper was essentially the proof of concept - the foundation for what’s happened since. Multiple independent labs across China, Italy, Germany, France, Canada, and the US are now publishing reproducible findings that converge on the same picture… The thoracolumbar fascia in people with chronic non-specific low back pain is measurably different - thicker, stiffer, and with restricted shear motion - than in pain-free controls.
The piece of the puzzle that remains unsettled is causation… In other words, does fascia dysfunction cause the pain, or does chronic pain (and the protective muscle guarding triggered by it) cause the fascia changes? Note that in Dr Langevin’s 15 year old experiment, the thoracolumbar fascia was imaged while it was in motion, although said motion was passive….
Now let’s look at the actual fascia itself (Reduced Thoracolumbar Fascia Shear Strain in Human Chronic Low Back Pain). What I want you to notice when you look at these videos is the huge difference between the chronic back pain subjects and subjects with no history of back pain…
Not only have these findings held up, but thanks to advances in diagnostic ultrasound technology and reproducibility & intra-rater reliability, they’ve been extended. For those interested, this list was composed by Claude (or feel free to skip it and get to the final chapter on…)…
A 2024 Frontiers in Bioengineering paper by Liu et al. found that in patients with chronic non-specific low back pain, the stiffness of the lumbar fascia and muscles is generally higher than in individuals without LBP, with the most significant changes observed in the L4-5 segments, and higher stiffness may be associated with pain and dysfunction, primarily manifested in the thoracolumbar fascia.
A 2025 follow-up study by Tomita et al. directly extended Langevin’s protocol with modern elastography and found higher TLF shear strain among individuals with non-specific low back pain than controls, between-group connective tissue differences, and positive correlations between elastography parameters and symptoms, indicating a potential link between TLF alterations and NSLBP.
Pirri et al. 2023 documented that compared to individuals without LBP, patients with chronic non-specific LBP exhibited significantly reduced anisotropy levels and increased thickness in the thoracolumbar fascia — a separate structural finding from the shear strain measurement.
A 2024 Pirri systematic review in Medicina surveyed the entire fascia ultrasound literature and noted that over the past decade, there has been a notable increase in research focused on ultrasound imaging of the thoracolumbar fascia, with US parameters including TLF thickness, echogenicity, stiffness, deformation, shear strain, and displacement.
A 2025 Scientific Data paper by Brandl et al. even released a validated phantom dataset for calibrating fascia ultrasound measurements — a sliding device with polyurethane tissue phantoms was developed to generate ground truth values for different distances and velocities, with 36 ultrasound videos for typical TLF sliding distances of 3-20 mm. This is the kind of methodological infrastructure that signals a field maturing.
BTW, I would love to have one of these advanced-tech diagnostic ultrasound units in my clinic. But only if you’re buying. The good ones, like those used in current research, are in the ballpark of half a million bucks.
Chapter 6: The Solutions
Notice that the title says solutions, plural. To reduce your chronic pain at its source is going to require some heavy lifting by you, proverbially speaking.
First, you’ll need to deal with systemic inflammation. Why? Because, as you saw in my previous post, inflammation always leads to fibrosis, the microscopic mesh-like web of tangled tissue that makes up a scar (emphasis on microscopic - it does not show with standard imaging). If you don’t turn the inflammation off at its source, it’s nearly impossible to get good long-term results. I’ve got a post on this subject that I wrote a dozen or more years ago. It’s not comprehensive but is as good today as it was back then.
Second, you will need to deal with the problem locally. What does that mean? It means that you’ll have to do something to address the abnormal function in your lower back. That dysfunction can either be sectional or segmental (or both), depending on what’s going on physiologically - or more accurately, pathophysiologically. There are about a jillion videos on YouTube on how to go about doing this. I’m a fan of lots of them.
Numerous different approaches to dealing with the local aspect of your problem work. but only if you’ve effectively dealt with the scar tissue / fascial adhesions of the thoracolumbar fascia and surrounding tissue. Find someone who is going to address that aspect of your problem.
Thank you Eva!
Wow wow wow I am so glad I found you a wee while ago (can’t remember whom cross referenced you sorry).
Both fascinating and incredibly well explained and illustrated.
And filled with hope.
Thank you