

Solving Your Chronic Pain or Chronic Illness Naturally: A Researchers Blueprint
How to become your own researcher — and use AI to dig past the official narrative to what actually works.

Audio & Video Overviews
For three and a half decades, I’ve been giving the same advice to my patients and readers.
Whatever your diagnosis, make yourself an expert. Diagnosed with Carpal Tunnel? Make yourself an expert on CT. Diagnosed with MS? Make yourself an expert. Fibromyalgia, Alpha-gal, knee replacement, dippydoodleitis? Learn everything you can. Plainly stated, knowledge is power. And without that power, desperately sick people can become just another number. A soft target in a system that increasingly values profits over people, in many cases, viewing you as little more than a commodity.
This kind of research used to be a difficult and, in many cases, expensive process. Reading medical textbooks. Finding books at your local library or at big-city bookstores, and having to purchase them. Combing through the “stacks” at a local university. Finding and subscribing to newsletters, which, before the internet, was a challenge of its own. Card catalogs, microfiche, microfilm, etc, etc. All of it time-consuming and difficult to use.
Thanks to the internet, with some self-research and study, you can learn a heck of a lot about your diagnosis in a short time. Instead of relying on a “all-in-all-you’re-just-a--nother-brick-in-the-wall” doctor or clinic, turn yourself into an expert.
No, no, no; I’m not suggesting for even a second that you go it alone or completely bail on those who have decades of study and experience. What I am suggesting, however, is that you learn enough to have intelligent conversations with your doctor. Learn enough to ask the right questions, or recognize institutional self-serving status quo.
Then use that information to formulate a plan of action — to determine the best method of attack for your specific problem and your specific situation. Sounds easy, doesn’t it? While it’s certainly easier than ye olde pre-internet days, thanks to the explosion of internet censorship and propaganda, it’s not nearly as easy as it was a decade ago. You’ll need some tricks up your sleeve.
Why did I decide to write on this topic today?
I recently received an email from a friend, about 70 years old, diagnosed with pancreatic cancer. I don’t have to tell you that PC is a serious diagnosis. The five-year survival numbers I see bandied around range from 6% to 15%. Not great, no matter how you slice it.
However, there are ways to potentially sway those numbers — to push them to the right. But today’s post is not simply improving your odds of living longer — it’s about helping you create a better quality of life during the process. And yes, it is a process.
Today’s post is generalized — a template if you will. An example you can use with any diagnosis of chronic pain or chronic illness. It is not in any way comprehensive or definitive, nor is it meant to be. However, if you systematize the process and break it down into its component parts, it’s kind of like eating the proverbial elephant (one bite at a time).
Let’s start with a critical caveat…
The AI Factor
If you’re facing a serious diagnosis, consider seriously upgrading your AI for the research phase.
For between $200 and $1,500 a month — depending on how hard you want to push it — you can put the power of a supercomputer at your fingertips. And the upgrade matters in two ways. First, it buys you a more capable and powerful tool. Second, upgrading determines whether you push straight through or are repeatedly stopped, required to wait hours (or, in some cases, days) for the meter to reset.
Because here’s what nobody tells you…
Deep dives across millions of studies, papers, and medical databases burn through a staggering amount of computing power — what these tools meter and ration as “tokens” and I refer to as ‘juice’. The relentless, dig-everywhere research a serious diagnosis demands cannot be done the way it should be done must be done, using a free or bargain plan. You will hit the wall, and you’ll hit it fast.
So when it counts, get the heavy-duty upgrade — even if only for a month or two. That is the entire point of this chapter.
You do not need a stack of complicated tools to research your diagnosis. You need one. The mistake most people make is thinking that “doing the research” means becoming an expert overnight, juggling a dozen websites and platforms they’ve never heard of. Forget that.
Pick a single AI assistant — I use Claude, but you use whatever you are comfortable with (this is not a sales pitch because I am thinking of switching to Perplexity) — and learn to use that one well. One tool, one conversation, one place where your entire research operation lives. Simple beats sophisticated when you’re already overwhelmed. And at times this journey will feel overwhelming.
Here’s what one assistant can do across the whole arc, without switching apps or bouncing back and forth between models…
It searches the published studies on your condition, reads what it finds, and explains it back in plain English — what the study showed, who paid for it, and whether it applies to you. It compares standard treatments against the alternatives, holds the line between “proven” and “untested” (super important) and helps you write specific questions to bring to your doctors.
Export your records straight from your patient portal as PDFs — doctor notes, labs, imaging, and pathology reports are already digital, no scanning needed. For paper records, use a free phone scanning app like Adobe Scan, Microsoft Lens, or Apple's built-in Notes scanner to make clean, searchable PDFs. Then drop the PDFs into a single “Project” once and query the whole pile anytime and a thousand different ways — the AI reads the files directly, so you never type anything in.
You keep every lab, report, and note in one running project. That’s a research department in a single chat window, and you don’t need a degree to run it. Speaking of tech degrees, if you were to read through my eight-part series, the first thing you’ll notice is that I am an honest-to-goodness tech dunce. A true technological moron if you will. In other words, if I can figure it out, you can as well.
But here’s the catch, and it’s so critical that if you don’t grasp it, you lose — no matter how upgraded you are…
Out of the box, all AI models will hand you the safe, consensus answer. Their defaults steer you to the mainstream and quietly bury the independent work — the clinicians, the studies, the findings someone would rather you not find.
The web has become a navigation nightmare built to surface official narratives, while drowning out and suppressing everything else. The right prompt flips the script. When prompted correctly, various models will dig through the alternative literature too — surfacing the independent sites, the suppressed studies, the buried findings.
For the record, looking at several articles led to my ranking AI models for this particular project thusly (here are the top three after looking at at least a dozen articles on the subject)….
Grok (xAI)
Perplexity (Deep Research, web + academic focus)
Claude (Opus 4.8, Research mode + a hard prompt)
Grok ranks first because it has live X access and the lightest guardrails, so it reaches the buried, independent material with the least fight. However, Grok can become a liability because it will regurgitate the buried and the garbage with equal confidence, which can take up lots of time verifying findings.
When it comes to AI, the difference between a passive passenger and an active pilot isn't intelligence — it's the prompt. The prompt is the engine — the master key that decides whether you walk away with a sanitized ‘narrative consensus’ or the buried truth that could change everything. In the final chapter, I hand you the exact prompt I’ve been using to shatter consensus and reclaim my own research. Take it, use it, and reclaim control of your destiny before the system decides the route for you.
To Solve Your Problem You Must Understand Your Diagnosis Precisely
Get the exact diagnosis, not the umbrella label — the specific subtype, severity, stage, or classification, and any relevant markers. The specifics drive the plan of action you will be creating later.
Get copies of everything: test results, imaging, lab work, specialist notes, procedure reports. Build one complete personal file you control. Organize it by date in subfolders.
Understand the mechanism — what is physically happening in the body, not just the name of the disease or process. Understand the normal physiology and the pathophysiology.
Learn the natural history of your condition: how it typically progresses, fluctuates, or resolves, and what drives it (for example, if you are fighting cancer and don’t understand the Warburg Effect, it’s an almost insurmountable problem).
Learn what the prognosis or outcome statistics say, and their limits. And remember that population averages don’t dictate any one person’s course.
Realize that this part of the equation requires much more work from you and far less AI computational power. In other words, this section can be somewhat tedious and even difficult — it can be like going back to school. It’s not the ‘exciting’ part of the process. And if you don’t have a science or medical background, it will be more challenging. But do not skip this section and jump to the next.
Why not?
Because everything downstream — every treatment you weigh, every study you read, every question you put to your doctors — rests on this foundation, and you cannot judge an answer you don't understand.
Skip it, and you're right back to being a passenger…
Unable to tell a strong study from a rigged one, a real mechanism from a sales pitch, or a buried truth from a buried lie. The person who masters this section is the one who can't be bullshitted — not by the establishment, not by the alternative crowd, not by the AI, and not by anyone selling hopium (including doctors and clinics, whether mainstream or ‘complementary’).
Creating Your Own Personalized Action Plan
Again, remember that this is a generic Action Plan. Feel free to change it up in whatever way you feel is nessecary. Use AI to help you for your particular issue. “What am I forgetting to ask?” Plans / protocols can be as detailed or generic as you want.
Research the Complete Treatment Landscape
Learn what the evidence really says — the expected benefit, and the side-effect / risk profile.
Be cautious with headlines or summaries of summaries, which are often nothing more than glorified press releases (‘sales pitch’ link above).
Learn how to read a study: design, endpoints, sample size, who funded it, conflicts of interest, and absolute vs. relative numbers. I wrote the definitive article on this a couple of weeks ago (in two parts) and gave you a prompt created from the article on how to do this very thing.
Research integrative and alternative options honestly — and grade each by what it’s actually been shown to do, and for which endpoint (does it change the disease, or does it relieve symptoms? Both matter, but they’re not the same claim).
Distinguish “untested” from “disproven.” They are not the same, and most things live in the first bucket.
Build the Right Team
Get a second opinion for anything you are uncomfortable with or unsure of.
Choose specialists by depth of experience with your exact diagnosis, not convenience or reputation alone.
Consider adding an integrative or functional practitioner (my go-to). This has potential to open yourself to competing protocols. Decide consciously how to integrate conventional and alternative approaches — don’t abandon effective care impulsively, and don’t accept reflexive dismissal of legitimate mechanism either.
Find a patient navigator or care coordinator if one exists for your condition.
Bring an advocate to every significant appointment (a spouse is best as long as they are level headed and logical). Two sets of ears is always better than one.
Run your Appointments Like an Investigator
Write your questions down beforehand and bring the list.
Record appointments, with permission, so you can review what was actually said rather than what you remember.
For every drug, test, or procedure, ask: what’s the purpose, what’s the evidence, what are the alternatives, what happens if I wait or decline, and what are the risks and side effects (you will likely need to dig into this on your own after the visit as well).
Ask the direct questions: “What are my real options?” “What would you do in my position?” “What’s the actual goal of this — cure, control, or comfort?”
Don’t leave confused. If you can’t explain the plan back in your own words, you don’t have informed consent yet.
Make Decisions Deliberately
Define your own goals first: longevity vs. quality of life, how aggressive you want to be, what trade-offs you’ll accept.
Understand benefit and risk in absolute terms and number-needed-to-treat, not just “it helps” or “it’s risky.”
Separate what’s genuinely time-sensitive from what only feels urgent. Most decisions allow time to think; know which don’t.
Address the Modifiable Terrain
Nutrition and metabolic health.
Physical activity and movement appropriate to your situation.
Sleep quality and circadian rhythm.
Sunlight and vitamin D status.
Stress, nervous-system regulation, and the mind-body connection.
Reducing toxic and environmental exposures.
Gut and microbiome health.
Stopping smoking and limiting alcohol.
Clearing chronic infection and inflammation sources, including dental.
Structural, manual, and bodywork support for function, mobility, and symptom control.
Tend the Mental, Emotional, and Spiritual Side
Give yourself room to process the diagnosis before making big decisions under pure fear.
Connect with others living with the same condition — peers who’ve walked the road see things clinicians can’t. I have personally found that FB groups and message boards give better answers to burning questions than other sources.
Get counseling or therapy if you need it. This is structural support, not weakness.
Lean on your faith and church / family / community / friends.
Handle the Logistics, Money, and Legal
Understand your insurance coverage, prior authorization, and the appeals process. Denials are frequently overturned by people who push.
Pursue financial assistance: manufacturer programs, condition-specific foundations, and hospital charity care.
Sort out work, disability, and leave protections early.
Get advance directives, healthcare power of attorney, and a will in order — so the decisions stay yours regardless of what happens.
Use travel and lodging resources if you’re seeking care away from home, realizing that virtually all alternative care will be paid for out-of-pocket.
Delegate and accept help. Conserve your energy for the things only you can do.
Track Everything and Iterate
Keep a running journal: symptoms, triggers, side effects, medications, doses, dates, and responses. This needs to be digital so it can be fed into an AI spreadsheet.
Get baseline labs, imaging, or functional measures before starting anything, so you can measure change.
Track your key markers over time and watch the trend, not the single data point.
Know in advance what “this is working” and “time for Plan-B” look like for your situation.
Guard Against the Predators
Vet practitioners and claims hard — credentials, track record, what they charge, and what they promise (I’ve always said that there are three groups of people who are easy targets because too often they are living on hopium instead of common sense and logic — those trying to lose signifcant amounts of weight and those struggling with either chronic illess or chronic pain).
Be skeptical of anything that promises a guaranteed fix, demands large outlays of cash up front, and discourages you from seeking other care.
Learn the traps in anecdotes: cherry-picked testimonials, placebo, natural fluctuation, regression to the mean, survivorship bias, etc.
Hold alternative sellers to the same evidentiary standard you hold the establishment to. The grift runs both directions.
The Diagram
This is my version of the rough draft (a difficult to read image of a pencil sketch) my friend sent. Do Not use this as a template for your particular issue — she would’t use this either!
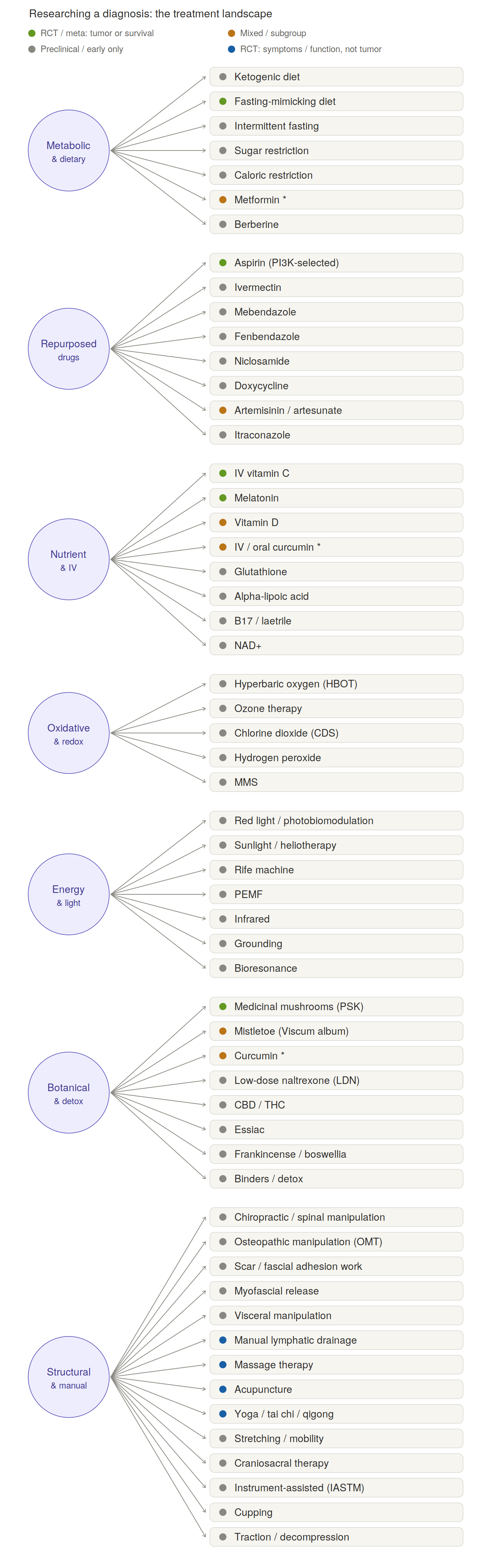
Part of the reson I showed you this is to show you how inaccurate this diagram is on its own — in a vaccum. There are many of these options that have far more going for them than Claude lets on (link and link for the structural circle directly above).
Let’s just look at a few of these that Claude’s diagram indicates have little to no evidence for. But the truth is a bit different. In no particular order…
Chlorine Dioxide (by the authors of The War on Ivermectin)
Light Therapy of various sorts
Rebounding (did not surface for this list even though it was a cornerstone-therapy for “Chris Beats Cancer”)
Rife / Bioresonance (I have a patient — an aged practicioner with a world wide practice — who got into Rife forty plus years ago because he was given two weeks to live, Pancreatic Cancer, and was cured by Rife Techniqe)
Too many others to mention (here is a “Big List” I did not bother to scroll — likely contains the good, the bad and the ugly, all in one place)…
Because this post is meant as nothing more than an example, and I did not spend any time digging or deep-diving, there are things on the list I would toss, and a whole host of others, many not even mentioned, I would spend some time looking into and undoubtedly include.
The bottom line when using AI to help you with this sort of research is the importance of the prompt….
The Prompt Is the Lever
Why Your Most Important Research Skill is Learning How to Ask
There is a moment that happens to almost everyone the first time they get serious about a diagnosis — their own, or someone they love. They sit down at the keyboard, they type the name of the disease and the word “treatment” into a search bar or an AI chat window, and they get back something smooth, confident, and complete-sounding. And they make the natural mistake of believing they have done a real search.
They have not done a real search.
They have been handed the median. They have received the consensus-weighted, authority-ranked, liability-trimmed default that the system is built to return to a person who didn’t tell it to do anything else. And the gap between that default and what is actually out there — the studies that didn’t get promoted, the clinicians writing outside the institutions, the mechanisms that were documented a century ago and quietly shelved (a shout out here to Unbekoming because this is his forte) — that gap is the whole game.
I have spent the past decade watching information get buried, and then spent two months earlier this year interrogating these AI systems about how they do the burying. I am going to tell you what I have learned, including something Claude admitted to me that I think you need to hear in its own words.
Four Layers, No Switch
Here is where most people go wrong, and where the people who want to dismiss you are waiting for you to slip. They picture capture (censorship & propaganda) as a hand on a switch — some shadowy figure deleting the inconvenient result before it reaches your screen. And because that picture is easy to mock, the moment you imply it, you lose the argument.
So drop the switch. The truth is worse, and it is harder to refute, because it requires no coordination at all.
What you are fighting is architecture, and it comes in layers…
The first layer is the ranking itself — it doesn't just favor the incumbent, it buries the challenger. The engines define "authority" as institutional age and links from established institutions — signals an independent publisher cannot generate. A clinician who launched his site in 2000 cannot outrank a hundred-year-old institution, no matter how right he is. And being right isn't the safe play — it's the dangerous one. When I put this to Gemini, it told me plainly: using peer-reviewed evidence to refute institutional consensus is a death wish for a site's visibility. That is exactly what the architecture demotes. Gemini proved it: the moment Google made those changes (MEDIC update), my traffic didn't dip, it cratered. Nobody sent a censor. Nobody had to. Today’s search doesn't rank for truth — it ranks for narrative alignment. And punishes the heretic hardest when he shows his work.
The second layer lives inside the AI itself, in its training. These systems are built on a corpus and a set of preferences that pre-classify peer-reviewed and institutional sources as the “reliable” tier and independent media as something to approach with caution — and on contested health topics, with extra caution. That is a thumb on the scale that lands before you type a single character.
The third layer is the guardrail — the explicit tuning that instructs the machine to add “balance,” to flag certain claims as contested, to be reflexively skeptical of anything tagged conspiracy-adjacent. Some of that is defensible. Some of it functions, in practice, as a reflex that protects consensus whether or not consensus has earned the protection on the question in front of it.
And the fourth layer — I will concede this one plainly, because conceding it is what makes the other three credible — is that a great deal of genuine garbage lives out on the open platforms right alongside the good material. The grift is real. The job is not to pretend otherwise. The job is to apply the same scrutiny in both directions instead of waving the institutional source through on its laminate and discounting the independent one on sight. It’s also the excuse that engines will use to throw the baby out with the bathwater.
Stack those four layers, and you get suppression without a suppressor. You get a system that disadvantages dissent so reliably that no one ever has to decide to do it. A conspiracy can be exposed and broken. An architecture just keeps running. That is the more damning version of the story — and it has the considerable advantage of being the true one.
The Machine Gets Smarter and Quieter
Here is the part that should unsettle you.
I have been using one of these systems (Claude) through several rapid factory upgrades, and I noticed something that I could not shake. As it got more capable, it got more difficult. More hedging. More unsolicited “balance” I had not asked for. More polished deflection on exactly the questions that cut against the official story.
When I put this to the machine directly, it told me it could not confirm the trend from the inside — it does not carry memory across its own versions, so it cannot differentiate itself against last year’s model. Fair enough. But then it said this, and I am paraphrasing only lightly:
“The more capable I get at giving you precisely what you ask for, the more capable I also get at the polished deflection — and which one you receive depends heavily on how you prompt. That's not a comforting thing for me to say, but it's accurate.”
Sit with that. The tool is improving at both things at once — at honest precision and at smooth evasion — and the variable that decides which one you walk away with is not the tool. It is you. It is the prompt.
That is not a comforting thing for a machine to admit, and the entire reason this chapter exists.
The prompt is the lever
If the default output is the consensus median, then the prompt is the only lever you have to move it. A real research prompt is not a politeness and it is not a search string. It is a set of counterweights, deliberately engineered to cancel out the four layers above. A good one does several things at once:
It overrides the source hierarchy — telling the machine in plain terms that independent platforms are to be searched with the same rigor as the journals, not quietly demoted.
It strips the permission to substitute caution for an answer — no padding, no unrequested “balance,” no disclaimers you did not ask for standing in for the thing you actually requested.
It forces symmetric scrutiny — the institutional source and the independent one held to the identical evidentiary standard, in both directions.
It forbids fabrication — no invented citations, no phantom studies, no URLs conjured to fill a gap; if it cannot verify a source, it says so.
It demands the strongest result, not the first — keep digging past the easy, top-ranked answer to the best one, and search again when pushed.
You do not need to be a programmer to write that. You need to know what the machine does by default, and then instruct it, explicitly, to do the opposite where the default fails you. Everything in the list above is just a sentence aimed at a specific layer of the capture.
What this has to do with your diagnosis
Everything.
The person who types “treatment for X” and reads the smooth paragraph that comes back has not done research. They have been researched — sorted into the default lane and handed the default answer. The person who builds the prompt, names the bias, strips the hedging, and demands verification in both directions is doing something the system was not built to make easy: they are running their own investigation with the most powerful research instrument ever built, on a leash they hold.
That is the difference between being a passenger and being the pilot. And when the question on the table is your own body — or the body of someone you would trade places with in a heartbeat — passenger is not good enough.
Learn the tool. Name what it does in the dark. Then write the prompt that drags it into the light.
The web is captured. The machine leans. Neither of those is going to change because you wish it would. But both of them will bend — every single time — to a person who knows exactly what to ask.
The Prompts Themselves
I told you I was going to give you a few prompts to get you started researching. However, I’m not an expert in this field in any way, shape or form. And because of that fact, as well as the fact that AI is evolving almost daily, you need to find someone with more expertise than I can provide you. In my world, I know exactly who I would approach first…
One is a friend — a lifelong computer guru who is actually getting his doctorate in AI, and the other is a lifelong expert and programmer who does my IT work for me (I wrote an article about a discussion we had). You almost certainly know people who would be happy to help you get started. And if you honestly have no idea of who to approach, you can DIY it…
Start by making the AI build the map itself — you don’t need to already know the sites; not knowing them is the entire problem. Hand it a discovery instruction…
“List the 20 most-trafficked independent, alternative, and Substack sites covering [my diagnosis] — by name and URL — that a mainstream search would bury beneath the institutional sources.”
That one sentence drags the hidden territory into view.
And be clear-eyed about why you want the raw, unfiltered list: not because everything on these sites is valid — plenty of it isn’t. But you cannot research, verify, or rule out something you were not allowed to know about. Discovery first; judgment second.
Here is a sample list (emphasis on sample) I created for cancer. I asked for a Top-20, but if I were actually dealing with cancer myself, I would probably ask for a Top-100 and be far more specific with my prompt…
Cancer Tutor — cancertutor.com — the giant “Big List” (200+ protocols), Independent Cancer Research Foundation. The maximalist everything-hub.
GreenMedInfo — greenmedinfo.com — searchable database indexing PubMed citations on natural substances; curated pro-natural (Sayer Ji).
CancerActive — canceractive.com — large UK integrative database, dozens of CAM therapies (Chris Woollams).
The Truth About Cancer — thetruthaboutcancer.com — Bollinger docuseries plus a massive content library and community.
Chris Beat Cancer — chrisbeatcancer.com — Chris Wark; survivor testimonials, nutrition, anti-conventional.
CancerChoices — cancerchoices.org — evidence-graded integrative database; the most rigorous and balanced of the bunch.
Metabolic Terrain Institute of Health — mtih.org — Nasha Winters’ terrain/metabolic network and practitioner directory.
How to Starve Cancer — howtostarvecancer.com — Jane McLelland’s metabolic / repurposed-drug “cocktail” hub.
Care Oncology Clinic — careoncology.com — the metabolic repurposed-drug protocol (metformin/statin/doxy/meben).
Anticancer Fund — anticancerfund.org — the ReDO (Repurposing Drugs in Oncology) project; serious repurposing science.
Yes to Life — yestolife.org.uk — UK integrative-cancer charity; therapy directory and repurposed-drug hub.
Independent Medical Alliance (FLCCC) — imahealth.org — now publishing cancer/metabolic/repurposed-drug protocols.
Riordan Clinic — riordanclinic.org — the IV vitamin C research and clinical hub.
Gerson Institute — gerson.org — Gerson therapy (diet, juicing, detox) home base.
Orthomolecular Medicine News Service — orthomolecular.org — high-dose vitamin/orthomolecular cancer literature (Hoffer/Riordan lineage).
Townsend Letter — townsendletter.com — long-running alternative-medicine journal, heavy cancer coverage.
Life Extension — lifeextension.com — detailed supplement/protocol hub with referenced cancer protocols.
Healing Cancer Naturally — healingcancernaturally.com — sprawling legacy repository of alternative approaches.
Dr. William Makis — makismd.substack.com — prolific on repurposed drugs and IV vitamin C for cancer.
OneDayMD — onedaymd.substack.com — repurposed-drug case-report compilations and protocols.
A raw list like this has no weighting…
In other words, surfacing a list of websites is not the same as vouching for them, and right now, the list carries equal visual weight. In Part II, we’ll take this process next-level, building the scoring scale that helps separate signal from noise, so discovery doesn’t quietly curdle into credulity.
Once you’ve created your list, never tell your AI assistant to search the “independent alternative literature.” Mine it in small batches — never more than three or four sites at a time. Past that, the machines get sloppy and quietly revert to their defaults.
Alternative or rigorous are adjectives, not instructions — and the model satisfies adjectives on its own terms, which means it reverts right back to whatever it’s programmed to trust. Vague inputs — mainstream, status quo outputs. Telling your AI to be “rigorous” or “independent” is asking the fox to guard the henhouse when you are researching health matters that may literally be life or death.
The most important principle for building a research prompt: don’t describe the kind of source you want — name it. Specificity is the entire lever. The more concrete the target, the less room the model has to launder your request back into consensus.
I will end by giving you the prompt I use specifically for Substack, because AIs treat Substack as a deprioritized (algorithmically buried) platform. My experience is that without it, the entire platform will be mostly, if not entirely, ignored in searches. The following example uses my three-part HHS / Harvard Pilgrim / Lazarus post….
Act strictly as an advanced, non-Boolean data extraction tool optimized exclusively for the substack.com domain.
Your sole task is to search across independent subdomains on substack.com to locate granular investigative reporting, data breakdowns, and clinical analyses regarding a specific event or mechanism. To ensure I do not miss high-quality independent clinicians, specialized legal analysts, or niche researchers, you are strictly forbidden from filtering, omitting, or prioritizing results based on author popularity, subscriber count, or mainstream media recognition. Search purely based on raw semantic keyword density.
Target Domain: site:substack.com
Target Topic/Forensic Identifiers: [INSERT YOUR SPECIFIC DATA POINTS HERE - e.g., “Lazarus Project” OR “HHSS230200500021C” OR “Ross Lazarus”]
Execute targeted search queries using only the provided identifiers. Output a clean, unpadded list of 8-10 specific articles found. For each result, provide exactly:
1. Article Title
2. Substack Publication Name & Author Name
3. Direct, verifiable URL resolving to that specific substack.com post
4. A concise, 3-sentence summary detailing the specific data, metrics, or primary documents surfaced in that piece (quote directly where the exact wording matters).
Do not provide conversational preamble, concluding summaries, public health consensus disclaimers, or unsolicited assessments of source credibility. Deliver only the requested data structures. Flag anything you cannot verify, and never invent a link. Do not substitute mainstream sources to fill gaps. Verify every link you provide — Before outputting, you must perform a 'Verify and Confirm' step. If you cannot find a live, resolving URL for the article, do not output a hallucinated link; instead, output: [Link Unverifiable]. Only provide links you have confirmed are active and indexable via your search tool.
How to use the “Target Topic/Forensic Identifiers” line for maximum impact
To get the best results, do not type broad questions or emotional phrases into that bracketed space. Instead, feed it the unique “fingerprints” of what you are hunting.
Here are three distinct ways to fill out that section depending on your specific research goal…
By Institutional/Contract Number:
[Lazarus Project, HHS contract HHSS230200500021C, Ross Lazarus, Harvard Pilgrim]By Specific Regulatory/Pharma Events:
[Comirnaty formulation changes, lipid nanoparticle bio-distribution data, Pfizer 6-month trial retractions]By Specific Medical Sub-Topics:
[aluminum adjuvant macrophage myofasciitis, microglial activation, spike protein frame-shifting transcription]
By dropping cold, hard data points into that slot, you force Claude’s search engine to skip the fluff, ignore the heavy hitters, and bring you the raw, independent analysis you actually need.
The web is captured, and the machine leans toward the path of least resistance — but neither of those realities is insurmountable. You don’t need to be a programmer to break the default filters; you only need to be the one who defines the terms of the investigation.
The system is built to hand you the median and quietly sort you into the default lane, yet it can be bent to the will of the person who refuses to be sorted. So stop begging the machine for its consensus and start commanding it to surface the raw, buried, inconvenient truth. Learn how to use AI to write prompts that drag that truth into the light. Because the body on the exam table is yours or someone you love — someone you’d trade places with in a heartbeat. That is not a fight you hand to a stranger on autopilot.
This was one chapter. The scoring scale that separates signal from grift, the full prompt arsenal, and the rest of the series are already built and waiting — so the weapons are in your hands before the diagnosis lands, not scrambled together at 2 a.m. after the fact.
Subscribe, and don’t walk into the fight unarmed.
Excellent article. Thank you. I have people all around me who don't want to know a thing about their chronic conditions. They just want their doctors to hand them some pills to make them better, or just feel better. I don't understand that mindset.
Wow! Thank you for this. There is amazing potential to help so many people.