

Shoulder Problems and their Relationship to Advanced Imaging (MRI)
What if people with no shoulder pain frequently have MRI findings as bad or worse than those who do?

Audio & Video Overviews
Chapter I: The Man Who Said the Quiet Part Out Loud
If you want to understand the problem with shoulder imaging in one sentence, you could do a lot worse than Dr. James Andrews, the most renowned orthopedic sports surgeon ever to pick up a scalpel. Andrews is the dominant name in American sports surgery history for a reason. For starters, he’s an athlete’s athlete… This is what Sports Illustrated wrote about him in a 2010 article, titled How Dr. James Andrews went from Sports Fan to the Sports Surgeon…
A former pole vaulter at LSU — as a junior, he won the conference championship with a jump of 15' 1 ½'' — Andrews inherited his love of sports from his father, Rheuben, who coached football and track in Homer, La., and his interest in medicine from his grandfather James Nolen, who was known as a healer in the woods of rural Louisiana, dispensing ointments and salves to anyone who came to him with a malady. "My dad and grandfather planted the two seeds," says Andrews. "Sports and medicine."
Over a career that spanned more than five decades (today is his 84th birthday - he retired in 2023), he’s said to have performed nearly 50,000 operations on a staggering roster of athletes, including Roger Clemens, Bo Jackson, Michael Jordan, John Smoltz, Jack Nicklaus, Drew Brees, Brett Favre, Troy Aikman, Charles Barkley, and too many others to count. He also trained more than 300 orthopedic surgeons who went on to shape sports medicine all over the globe.
So when a man of that background — a man whose entire livelihood depended on operating on elite athletes, a man who performed as many as 50 surgeries a week — stands up at an elite sports medicine conference in front of 400 colleagues and delivers a warning about the overuse of imaging, you can’t help but listen. The lecture - “What I Have Learned About the Shoulder in the Past 30 Years” - could have been a victory lap. Instead, it was a confession.
Out of curiosity, Andrews had scanned the throwing shoulders of 31 healthy professional baseball pitchers that had come to see him for other problems. In other words, these pitchers had no pain, no injury, no symptoms of any kind. The MRIs showed abnormal shoulder cartilage in 90% of them. Abnormal rotator cuff tendons in 87% of them. These were not broken-down veterans. These were active, functioning major league pitchers doing their jobs at the highest level of professional sport.
Here is what Andrews told that room, and what New York Times science journalist Gina Kolata reported in 2011… Andrews’ conclusion, delivered in his characteristically plain Louisiana drawl, became one of the most quoted lines in the history of sports medicine: “If you want an excuse to operate on a pitcher’s throwing shoulder, just get an MRI.”
Read that again. The greatest sports surgeon in American history — a man who made his fortune operating on men whose shoulders earned them tens of millions a year — told a room full of his peers that MRI findings in the shoulder were, in his experience, essentially an excuse generator, and that improvements in imaging technology had given too many surgeons what he called “itchy scalpel fingers.” What if this same scenario were true across the entire body? And not just for athletes but for everyday Joes or Jolenes?
Not surprisingly, I’ve seen this phenomenon play out time and time again in my practice. One of my earliest examples came from a patient we’ll call Leroy. Leroy ran heavy equipment for a government entity, and one day, nearly five years before I saw him, slipped in the mud while getting on his loader. His feet flew out, and he fell. But he did not fall far because he kept hold of the handle used to pull oneself up into the cab. Needless to say, the one shoulder absorbed all that force, pulling it backwards as he twisted in the breeze.
He knew immediately he had done something bad to his shoulder. In the years that followed, he went to doctor visit after doctor visit, going thru round after round of therapy. He tried everything, finally coming to see me after someone in his neck of the woods told him he should. He was 80% better after a single treatment. I think I ended up doing a couple more.
I learned a valuable lesson from Leroy. He told me about the things that the doctors thought was wrong with his shoulder. But in his case, nothing showed up on his scans to justify a surgery (which in the end proved good for him). He not only got better, he got better quickly - almost immediately. And kind of like we saw in the last post on asymptomatic back pathologies (“Visualize Your Pain”), I am not the only one talking about the problems in the world of shoulder imaging…
Chapter II: Tens of Thousands of Studies, and They All Say the Same Thing
My PubMed search of “subacromial impingement syndrome” returned 3,000 results. One term on a single database. Expand the search to the full cluster of related diagnoses (we’ll discuss them in the next chapter), with a single Systematic Review returning over 23,000 results before filtering. The total number of peer-reviewed studies on shoulder pain, imaging, and related diagnoses runs into the hundreds of thousands, making it one of the most studied areas in all of musculoskeletal medicine.
But here’s what makes this research literature so extraordinary, and so relevant to what I showed in my previous post on non-specific back pain. The studies don’t just accumulate, they converge. Thirty years of research by thousands of independent teams around the world, dealing with different populations and using different types of imaging, and the central finding keeps coming back the same… What you see on a shoulder MRI does not reliably tell you who is in pain, who will develop pain, or who needs surgery. If that sounds familiar, it should because it’s the shoulder’s version of the same story (see previous link).
Shoulders that look “damaged” on imaging in people who feel completely fine appear equally “damaged” in people with pain. Doctors cannot reliably tell these groups apart from scans. That’s not me saying that, it’s the science itself that’s making this audacious claim. Here are five studies, across three decades, that make the case as clearly as it can be made.
In 1995, researchers at the University of Miami published what became the foundational study on this question, Abnormal Findings on Magnetic Resonance Images of Asymptomatic Shoulders. The authors scanned the shoulders of 96 people who had never had shoulder pain, shoulder problems, or any upper extremity symptoms whatsoever, discovering that rotator cuff tears showed up in just over a third of them (full-thickness tears in 15%, partial tears in 20%). In the 60+ crowd, over half had visible tears on MRI despite no pain and no functional limitation. The study’s conclusions were unavoidable. A rotator cuff tear on MRI is not inherently a diagnosis of anything. In many cases, it is simply what a shoulder looks like as it ages.
Four years later, a German research team published Age-Related Prevalence of Rotator Cuff Tears in Asymptomatic Shoulders, an ultrasound study of over 400 asymptomatic volunteers. Full-thickness tears turned up in nearly a quarter of them, with the numbers escalating steadily by decade: 13% in their 50s, 20% in their 60s, 31% in their 70s, and 51% in those over 80. The authors stated it plainly, “Rotator cuff tears must to a certain extent be regarded as normal degenerative attrition that does not necessarily cause pain or functional impairment.” The question of what actually converts an asymptomatic tear into a symptomatic one, they admitted, remained completely unanswered.
In 2013, Japanese researchers took this question into the real world in Prevalence of Symptomatic and Asymptomatic Rotator Cuff Tears in the General Population: From Mass-Screening in One Village. The authors used diagnostic ultrasound to screen both shoulders of 664 residents of a single Japanese village. Drum roll, please… Full-thickness rotator cuff tears were found in 22% of the 1,328 shoulders, with nearly 2/3 being completely asymptomatic. No tears were seen in participants in their 20s, 30s & 40s. However, by the time residents reached their 80’s, nearly 37% had visible tears. This shows that in the general population, having a confirmed rotator cuff tear on imaging is more likely to mean nothing than it is to explain your shoulder pain.
By 2016, researchers shone this same light on the labrum in a study titled High Prevalence of Superior Labral Tears Diagnosed by MRI in Middle-Aged Patients with Asymptomatic Shoulders. The authors used MRI to scan 53 people aged 45–60 who had zero shoulder symptoms. Radiologists diagnosed superior labral (SLAP) tears in 55–72% of them (no differences based on age, sex, dominant arm, physical job history, overhead sports, etc). What does that really mean? If a shoulder MRI in a completely pain-free middle-aged person will be read as a SLAP lesion over half the time, the diagnostic and surgical bar for labral pathology in patients who do have symptoms needs to be considerably higher than it is.
Then came 2025 and 2026 — two landmark studies published three months apart, in the last six months…
The first, Rotator Cuff Imaging Abnormalities in Asymptomatic Shoulders: A Systematic Review, crunched the data in 53 studies (3,800 patient records), finding that rotator cuff imaging abnormalities in asymptomatic shoulders ranged from 0–100% depending on age and imaging modality, with MRI showing tendinopathy or partial tears in up to 100% of certain asymptomatic populations. “Across studies with low- to very low–certainty of evidence, the prevalence of rotator cuff imaging abnormalities in asymptomatic shoulders ranged from 0% to 100%.” Numbers like that elicit about as much confidence as the distinguished radiologist, Dr AE Neuman, reading my scan!
The second study (the famed FIMAGE study out of Finland), Incidental Rotator Cuff Abnormalities on Magnetic Resonance Imaging, looked at both shoulders of 600 adults, using state-of-the-art 3-Tesla MRI. The results were shocking… Rotator cuff abnormalities were present in 96% of asymptomatic shoulders and 98% of symptomatic shoulders. Read those two numbers side by side. The difference between a shoulder that hurts and one that doesn’t, as seen on MRI, is essentially nothing.
The findings of this study suggest that rotator cuff abnormalities are nearly universal after age 40 years and that routine imaging should not guide diagnosis or treatment of non-traumatic shoulder pain.
Thirty years. Thousands of studies. Five continents. And the answer keeps coming back the same.
Chapter III: The Diagnosis That Swallowed the Shoulder
We are going to spend this chapter talking Subacromial Impingement Syndrome (SIS). What exactly is “shoulder impingement”? It honestly depends on who you ask. That’s because “impingement” is not so much a specific diagnosis as a catch-all term for a spectrum of overlapping shoulder pathologies (I call these “Bucket Diagnoses” - Not sure? Just throw it in the bucket labeled SIS - doubly messy in a world full of MUPS).
Some of these include…
Rotator cuff tendinopathy / tendinosis — chronic degenerative changes in one or more of the rotator cuff tendons, most commonly the supraspinatus
Partial-thickness rotator cuff tears — incomplete tearing of the tendon, often the articular or bursal surface of the supraspinatus
Full-thickness rotator cuff tears — complete disruption through the tendon thickness
Subacromial bursitis — inflammation of the bursa that cushions the tendons from the bony acromion above
Calcific tendinitis — calcium deposits within the rotator cuff tendons causing local inflammation and pain
Biceps tendinopathy — irritation or degeneration of the long head of the biceps tendon where it runs through the subacromial space
Painful arc syndrome — pain specifically in the 70°–120° arc of arm abduction, considered the clinical hallmark
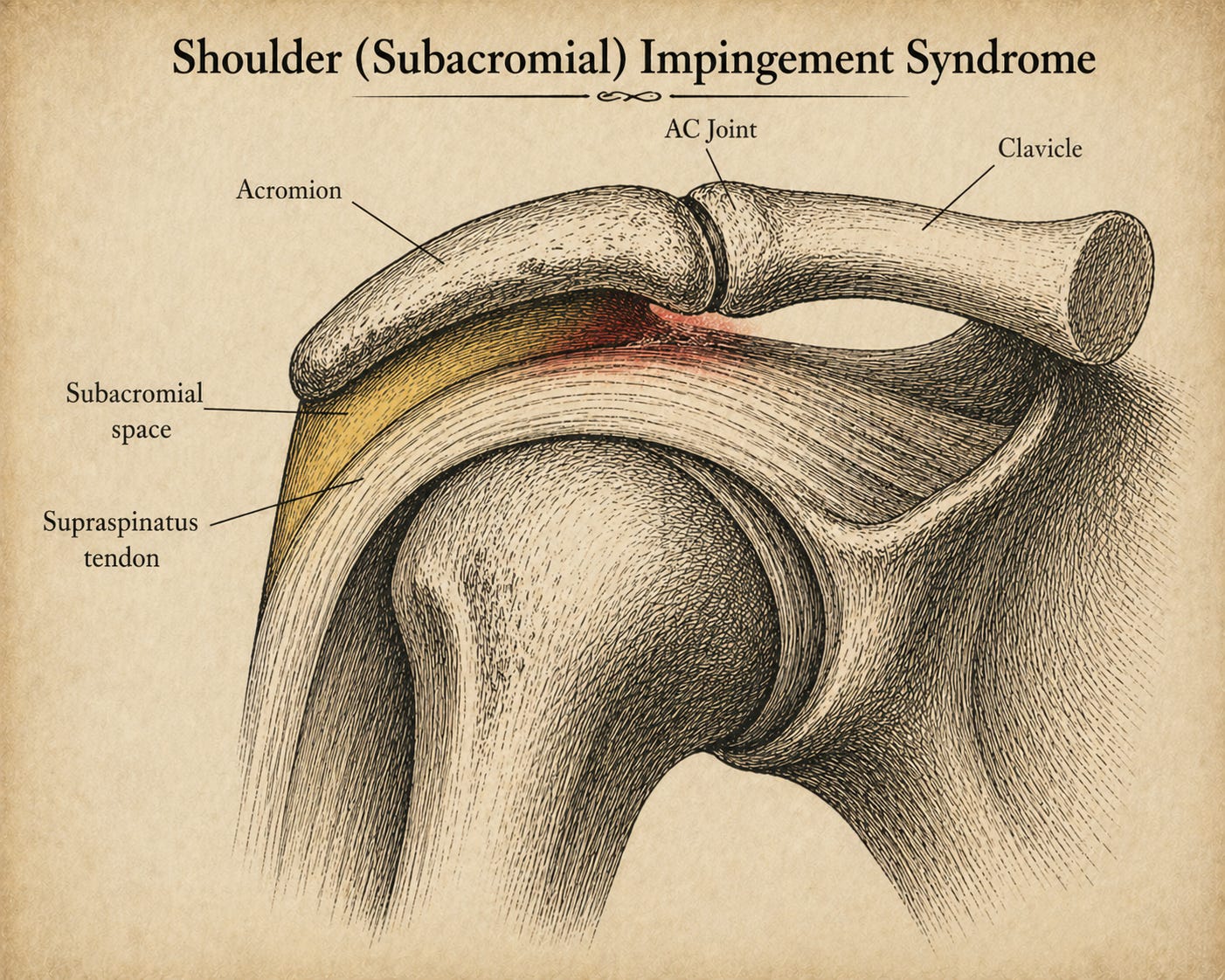
Supraspinatus impingement — the most classic version, where the supraspinatus tendon is compressed between the humeral head and the underside of the acromion
Scapular dyskinesis — abnormal scapular movement patterns that reduce the subacromial space during overhead motion
Superior migration of the humeral head — upward creep of the humerus due to rotator cuff weakness, further narrowing the subacromial space
Acromial morphology abnormalities — particularly a Type III (hooked) acromion, which physically encroaches on the subacromial space
AC joint osteophytes / spurring — bony spurs from the acromioclavicular joint that crowd the space from above
The symptom profile associated with this list includes pain, weakness, and loss of movement at the affected shoulder; pain worsened by overhead movement and commonly occurring at night (especially when lying on the affected shoulder); pain described as dull rather than sharp; and persistent, grinding or popping sensations (crepitus / creep) during shoulder movement.
It’s here that the impingement story takes its most uncomfortable turn…
The two physical exam tests most commonly used to diagnose this condition in the clinic — the Neer sign and the Hawkins-Kennedy test (with my all-time favorite illustration - try not to laugh) — have a specificity averaging around 50%, with meta-analysis showing that neither has meaningful diagnostic utility for impingement syndrome. That means that the two tests most frequently used to confirm the most common shoulder diagnosis in medicine are, statistically speaking, no better than flipping a coin.
And when researchers turned their attention to surgery — specifically the various acromioplasty procedures for shaving away the bony impingement in hopes of widening the subacromial space (pics coming momentarily), multiple studies have shown it to be no better than conservative treatment, and in the most rigorous trial, no better than sham surgery. Some authors in the peer-reviewed literature have gone so far as to call subacromial impingement syndrome a “medical myth” and “clinical illusion,” with calls to abandon the term entirely.
So what are we really left with?
A diagnosis that accounts for up to 85% of all shoulder pain, that globally generates an enormous amount of surgical revenue, whose two signature diagnostic tests cannot reliably confirm it, whose scans are as likely to mislead as to inform, and whose signature surgical treatment cannot reliably fix it. And the kicker is that over and over, the peer-reviewed literature makes the point that the underlying SIS model is, at a minimum, incomplete. Sound familiar? It should. It’s the shoulder version of my recent post on non-specific back pain.
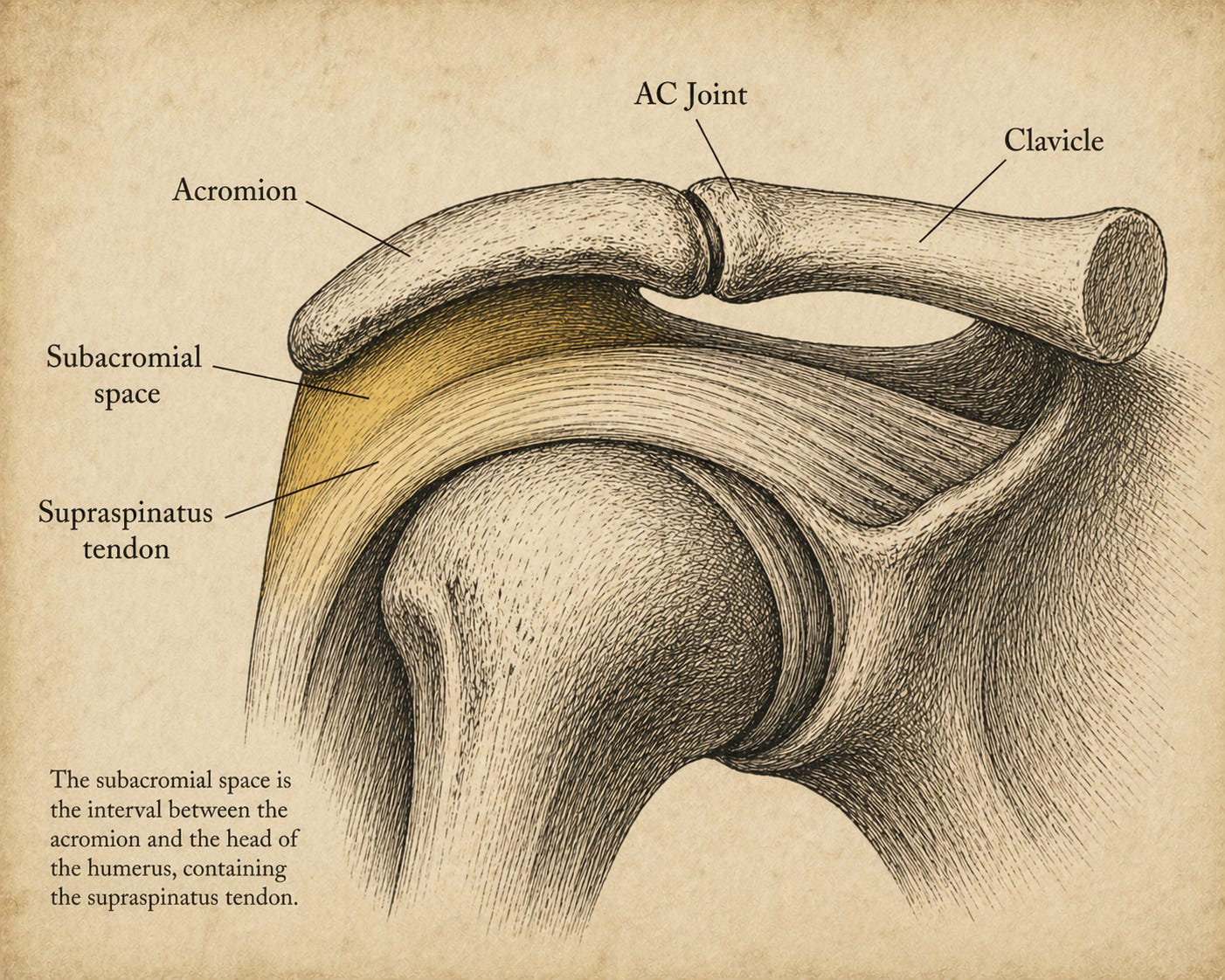
The shoulder is overwhelmingly soft tissue. The rotator cuff is four muscles — supraspinatus, infraspinatus, teres minor, subscapularis — whose tendons converge around the humeral head to form a dynamic stability sleeve, surrounded by a bursa, ligaments, the labrum, and the biceps tendon. Yet the dominant diagnostic framework for shoulder pain for the past 150 years has been a structural, bony one… A hook-shaped acromion, a bony spur, or a narrowed subacromial space, pinching the soft tissue and causing pain. The peer-reviewed literature has grown increasingly clear that this model is, at minimum, incomplete. So if it isn’t the bony architecture driving the problem, what is?
Here’s where the back pain story and the shoulder pain story converge…
Soft tissue, in the setting of chronic inflammation, overuse, and repetitive microtrauma, does something very specific and very predictable — it thickens, stiffens, and develops what researchers now call densification: the transformation of pliable, well-hydrated tissue into something that glides poorly, irritates adjacent nerve endings, and restricts motion in ways no bony decompression will ever address.
The rotator cuff lives inside a web of fascia and connective tissue spanning the entire shoulder girdle. When that web is compromised, the shoulder hurts. When it heals, it doesn’t. The MRI — excellent at showing bone and gross structural tears — isn’t designed to see any of this. That, more than anything else, is why the scans keep coming back looking terrible in people who feel fine (or vice versa), and why treating what the scan shows so often fails to make the pain go away.
Chapter IV: Before You Sign the Consent Form — Four Things Worth Trying First
Because, as you’ve seen, it’s a challenge to look at imaging and determine who has pain and who doesn’t, it almost always behooves us to see what can be done to solve the problem conservatively. Especially in light of Dr Andrews’ revelations on MRIs of the shoulder being used as surgery funnels rather than a diagnostic tool.
#1) Systemic Inflammation:
Deal with it. If you do not treat underlying inflammation, you will struggle to improve. It’s simply because, as I showed you in an earlier link, any amount of inflammation over what’s considered necessary for healing (an example of the MED principle) always leads to fibrosis. There are many therapeutic approaches that work, but regardless of which one you choose, you will have to make some changes in the way you live. Expect some challenges along the way, but diet and lifestyle modification are key to this bullet point.
#2) Deal with the Scar Tissue / Fibrosis that’s Already Present:
I cannot even begin to tell you about the number of patients I’ve seen over the years who were headed to surgery, and our tissue remodeling saved the day for them. Despite whatever doctors have told you is wrong with your shoulder, if the scar tissue / fibrosis side of the equation is significant, you have to deal with it, or it will remain “tethered” (shackled, fettered, strangled, choked, restricted, bound) despite your best intentions. In my clinic, you will know after a single treatment if this approach is going to help.
#3) Stretching & Dead Hanging:
In Outlive, Dr. Peter Attia names the dead hang as one of his four foundational strength and longevity exercises. But everything in the dead hang/shoulder literature traces back to one orthopedic surgeon, Dr. John Kirsch, who concluded that without regular overhead activity (i.e., some kind of hanging), the space between the acromion and the humerus undergoes slow contracture, producing the degenerative changes that underlie impingement, osteoarthritis, frozen shoulder, and soft tissue tears of the rotator cuff and labrum.
Kirsch is not a patient who stumbled onto something. He’s a board-certified orthopedic shoulder surgeon who spent three decades opening shoulders for a living. When he was diagnosed with a full-thickness supraspinatus tear, he knew the surgery, the recovery, the outcomes, and the statistics better than virtually anyone alive. And he said no. He grabbed a bar and started hanging. Within months, his pain was gone, his function restored, and the consent form in the trash.
Do not underestimate what it means when the expert refuses his own standard of care!
Kirsch then documented his findings with CT scans, treating 92 patients facing shoulder surgery with a hanging protocol and watching 90 of them cancel their procedures. He submitted the research for peer review in 2004 but was rejected. So he self-published. Meanwhile, the establishment that rejected his paper performs hundreds of thousands of acromioplasties a year — a surgery that, as we’ve established, performs no better than placebo. But no one was interested in his study on dead hanging as a potential solution for what is unarguably the majority of shoulder issues.
Kirsch offers a short, inexpensive paperback, based on his study, and offering utterly simple advice. It’s clear his motivation is not purely financial. What made this click for me, though, wasn’t a book or paper; it was people.
My brother, a Kansas farmer and ER physician, had a bad enough shoulder that he hadn’t thrown a ball overhand in 30 years. Two months of dead hanging, and he could throw again. A radiologist I treat (ugly imaging, scheduled for surgery) started hanging on my recommendation. A week later he called me to let me know he had canceled the procedure. Those kinds of turnarounds don’t come from healing a tear or lifting the acromion. Something changed functionally, and changed fast.
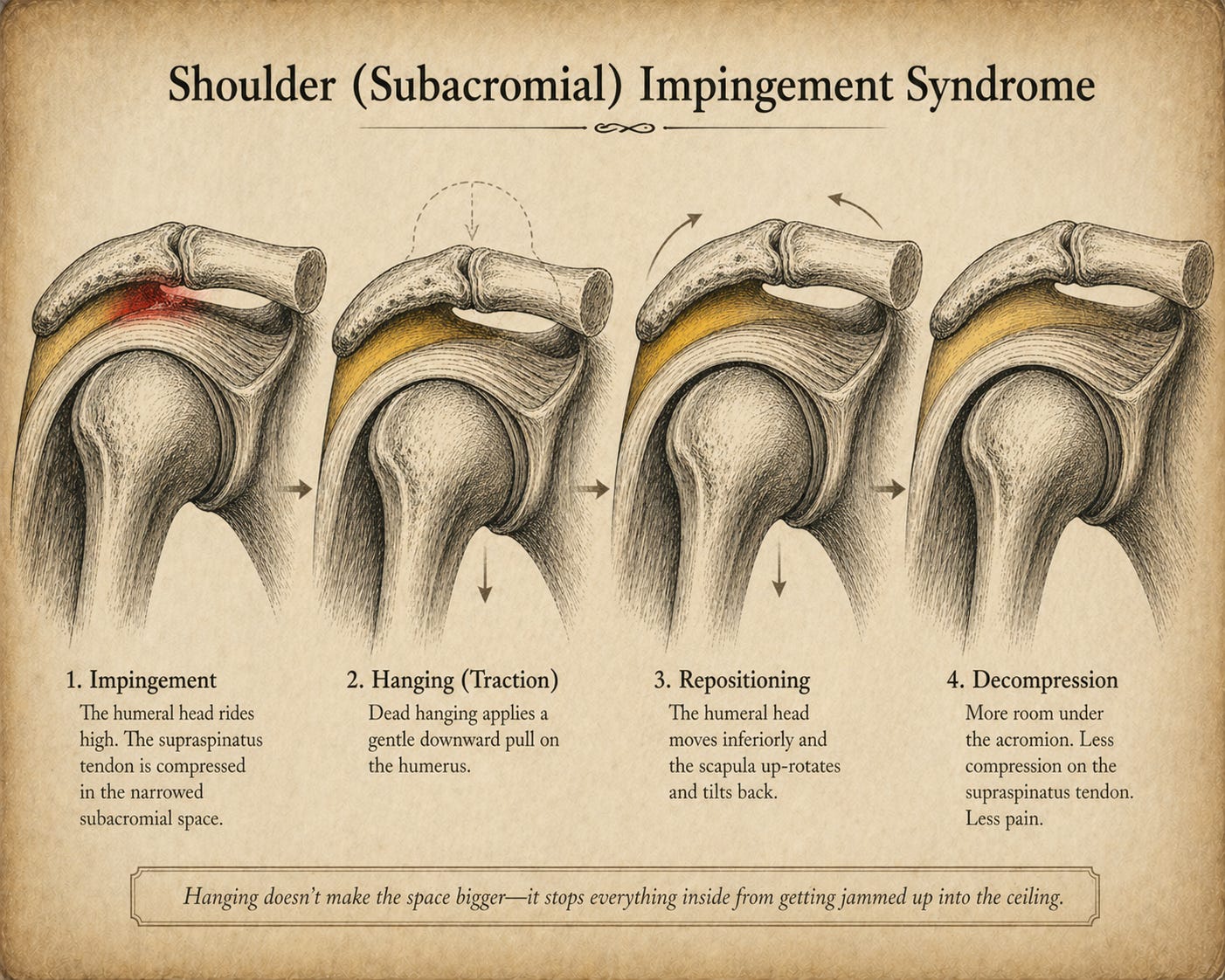
In a lot of “impingement” cases, the acromion hasn’t dropped; the humeral head is riding too high from muscle weakness and overuse, crowding everything above it. The supraspinatus and its neighbors get caught in the middle. Hanging ultimately pulls the humeral head downward, lets the shoulder blade rotate into a better position, and takes pressure off the cuff — the reason it often works so quickly. While we can spend hours debating what dead hanging is doing to the shoulder structurally, it’s not debatable that hanging does some very nice things to the shoulder functionally speaking.
There may, however, be even more to dead hanging than meets the eye — there may be actual bony remodeling of the acromion taking place when given enough time. What do I mean?
Kirsch makes that claim, verified by scans (see his book), showing that bony remodeling of the acromion can take place as a result of dead hanging (it raises upwards - which is interesting because studies have shown that some acromion shapes are more problematic than others). And honestly, if one sticks with it, why wouldn’t it? It’s simply Wolff’s Law in action. It’s the exact same phenomenon that causes impingement, working in the opposite direction. We can see an example in the textbook commonly called ‘the Bible of shoulder surgery’….
“Other studies have suggested that type II and III acromia are acquired rather than developmental.” -Rockwood and Matsen’s The Shoulder, 5th Edition
My copy of Kirsch’s book is currently loaned out, but I wrote an article on this years ago — great images — and if you struggle with shoulder issues, go back and study the preceding links.
#4) Strengthening Protocol:
I’m going to sound like a broken record here. Make yourself an expert on your problem. Watch a boatload of YouTube videos (I’d send you elsewhere, but the selection is too limited), and start taking notes. There are some amazing shoulder strengthening protocols out there, and most are free. My biggest recommendations here are simple — create a written plan, and when you start working that plan, add one or two exercises at a time. Why? If your protocol has ten exercises, nine of them might be perfect for you. But you will never figure out which one is not if you do it all starting on day one.
A Final Note on Frozen Shoulders:
I’m not completely sure what to make of frozen shoulder syndrome (Adhesive Capsulitis), as the scientific literature is all over the place, both as to what it really is, as well as the best treatment protocols (see link). Because I think it is more of an inflammatory condition than mechanical, #1 above is more than appropriate. However, when it comes to treatment and rehab, realize that while some people do great with the intense protocols, for others it can be aggravating to the point of debilitating. So proceed with caution (and look for a future post on this topic).
….. add DMSO for the win as well 😁
I have a bone spur in my left shoulder.
Dead hanging helps with yoga breathing.